
記住我
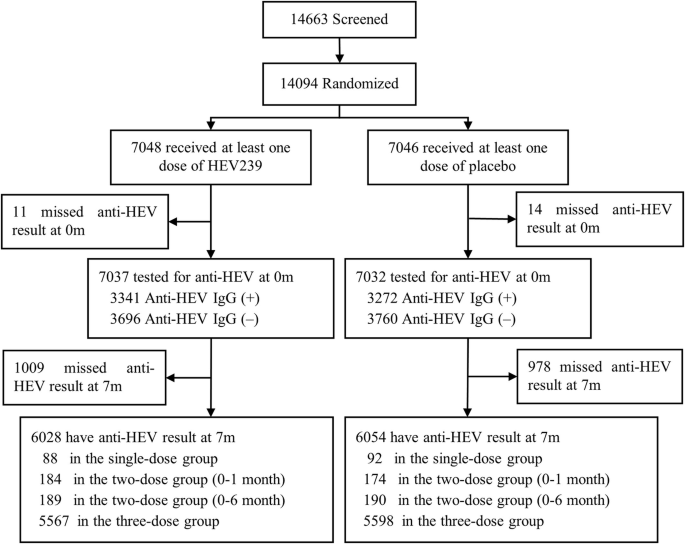

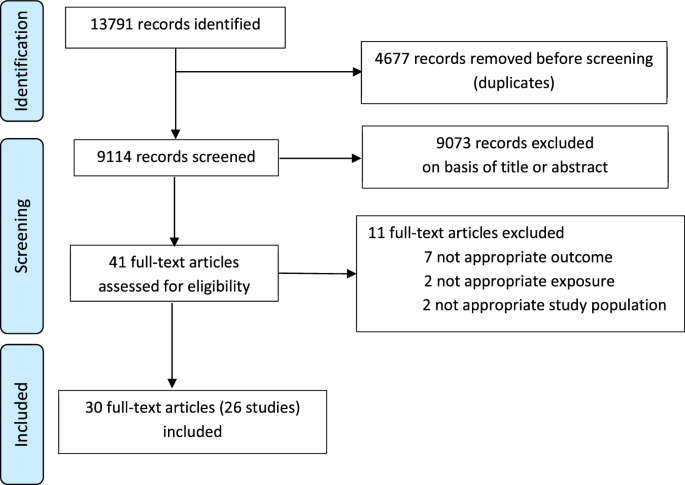
In total, 9114 records were identified. Of these, 30 (accounting for 26 studies) fulfilled the inclusion criteria and were included in the final analysis21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50 (Fig. 1). The characteristics of the studies are summarised in Table 1. Fourteen studies (16 publications) were done in infants and 12 (14 publications) in adults. Nine publications included less than 50 participants, 16 between 50 and 200 and 5 more than 200 participants. Most publications were from studies done in Asia (16 publications), mainly India, Bangladesh, and China, followed by Europe (6 publications), Africa (5 publications), North America (5 publications), New Zealand (2 publications), and South America (1 publication). Most of the studied vaccines were oral: rotavirus (ORV, 8 publications), poliovirus (OPV, 4 publications), cholera (OCV, 2 publications) and Salmonella typhi (1 publication). The remainder were parenteral: SARS-CoV-2 (7 publications), PCV, (3 publications), IIV (2 publications), and meningococcus C polysaccharide vaccine (MenC), poliovirus (IPV), tetanus, pertussis, DTaP/Hib (all together), hepatitis B (HBV) vaccines (1 publication each). To assess vaccine responses, most studies measured serum or plasma immunoglobulin (Ig) G (18 publications) or IgA (10 publications, all to ORV or OCV), followed by T-cell responses (5 publications), intestinal IgA (2 publications, OPV) and saliva IgG (1 publication). Stool samples were collected at different time points, but all studies included at least one sample before the first vaccine dose. Studies in infants collected the first stool sample between birth and 6 weeks of age (except one study investigating OPV in which stool samples were collected at 6 months of age). The stool analysis techniques used included 16S rRNA gene sequencing (18 publications), bacteria-specific polymerase chain reaction (PCR) (7 publications), shotgun metagenomic sequencing (10 publications), Human Intestinal Tract Chip (2 publications) and bacterial culture (1 publication). Seven publications used more than one technique.
Fig. 1: Selection of studies.
Flow diagram of identified, screened and included studies and articles, according to PRISMA guidelines.
Table 1 Summary of findings of studies investigating the influence of the intestinal microbiota on vaccine responses (significant findings are indicated in bold)All included publications had an overall risk of bias score (JBI standardised critical appraisal checklist, yes%) over 60% (acceptable quality), and 80% (24/30) of publications had an overall score ≥80% (good quality) (Supplementary Table 2). The most frequent risk of bias was a lack of identification of confounding factors and strategies to address these (present in 57% (17/30) studies). Some studies did not describe clearly how many children completed follow-up or the reasons for lost to follow-up. In some of the adult studies, ≥4-fold increase in antibody levels were used to overcome the difficulty of including seronegative or vaccinated naive subjects.
In total, 87% (26/30) of the publications reported an association between the composition of the intestinal microbiota and vaccine responses, though 3 of them found only an association with alpha or beta diversity and not with relative abundance of specific bacteria. We did not observe important differences between the studies assessing oral vaccines and those assessing parenteral vaccine responses. The findings are summarised in Tables 1 and 2, and in Supplementary Table 3.
Table 2 Associations between the composition of the intestinal microbiota at different taxonomic levels and vaccine responses (colour coding: higher relative abundance associated with higher vaccine response (blue); lower vaccine response (yellow), inconsistent findings (grey); all p < 0.05)Oral vaccinesSix publications in infants26,27,28,36,37,39,42 and one in adults29 reported on the association between the composition of the intestinal microbiota and serum IgA response to ORV, defining high responders as an IgA titre of ≥20 IU/mL or a ≥4-fold increase in titre (Tables 1 and 2). Five studies used the monovalent ORV vaccine27,28,29,37,39 and three the pentavalent26,36,42. Two publications reporting findings from the same study found a lower alpha and beta diversity of the intestinal microbiota among responders, but only in India and Malawi and not in the UK36,42. In the other studies, a higher relative abundance of Bacillota, Ruminococcaceae and Peptostreptococcaceae, Streptococcus bovis and Faecalibacterium prausnitzii and a lower relative abundance of Erysipelotrichaceae and Clostridium XVII were associated with ORV vaccine responders (all p < 0.05)27,28,29. Furthermore, a higher relative abundance of Pseudomonadota (Escherichia coli and Serratia), and Bacteroidota (Porphyromonadaceae and Prevotellaceae, and Bacteroides thetaiotaomicron) were associated with responders (p < 0.05), while for Bacteroides and Prevotella contradicting findings were reported27,28,29,39. A lower relative abundance of Fusobacteriaceae was also associated with higher vaccine responses (p < 0.05)29. One study found no association between the diversity or composition of the intestinal microbiota, but responders more often had more than one bacterial enteropathogen (26 vs 13%, p = 0.006)37.
Responses to OPV were assessed in 5 infant studies23,31,32,38,41, one of them using a subgroup of participants from a larger study31,32. Vaccine response assessment included polio-specific intestinal IgA, serum and plasma IgA and IgG titres, as well as T-cell responses23,31,32,38,41. Only one study found an association between a lower alpha and beta diversity and higher vaccine responses (intestinal polio-specific IgA, p < 0.05)41. Other studies reported that a higher relative abundance of Actynomycetota (from phylum to family level) and a lower relative abundance of Bacillota (from phylum to species level) and Pseudomonadota (from order to species level) were associated with higher OPV vaccine responses (p < 0.05)31,32,41. Exceptions to this were an association between a higher relative abundance of Enterococcaceae (Bacillota)32,41 and lower relative abundance of Bifidobacterium breve (Actynomycetota)31 with higher OPV vaccine responses (p < 0.05). A higher relative abundance of Prophyromonadaceae (Bacteroides) was also associated with higher OPV vaccine response (p < 0.05)32. One study found no association between the relative abundance of specific bacterial taxa in the intestinal microbiota and polio-specific serum IgG responses38.
Two studies investigated the association between the composition of the intestinal microbiota and OCV responses (plasma IgA and IgG ≥4-fold change in titre) in adults22,46. One study reported a higher beta diversity (UniFrac distances, p = 0.044) and vaccine response among high OCV responders46. These studies found an association between a higher relative abundance of Clostridiales22, Shigella, Anaerobaculum mobile and Bacillus licheniformis46, a lower relative abundance of Enterobacteriales22 and Bacteroides46, and higher memory B cell responses (p < 0.05).
Another study in adults found a higher alpha diversity and phylogenetic diversity with a higher relative abundance of Clostridiales (Lachnospiraceae and Ruminococcaceae) was associated with multiphasic cell-mediated immune response after an oral Salmonella typhi vaccine (p < 0.05). No association between the composition of the intestinal microbiota and serum IgA or IgG response was found25.
Parenteral vaccinesThree infant studies analysed the effect of the composition of the intestinal microbiota on the response to PCV24,33,43. The first study found no association between PCV vaccine response and intestinal microbiota diversity or composition43. The second study found that a higher relative abundance of Escherichia/Shigella, Bifidobacterium, Bacteroides, Ruminococcaceae, and Streptococcus bovis (adjusted p < 0.05) and a lower relative abundance of Bacillota, Enterobacteriaceae, Prevotella, Bifidobacterium bifidum and Garnerella was associated with higher pneumococcal-specific saliva IgG levels (adjusted p < 0.05)24. The third study found no association between the beta diversity of intestinal microbiota or the abundance of specific taxa and serum pneumococcal IgG titre33. The second study also investigated the association of the intestinal microbiota composition at 2 and 12 months and meningococcal-C saliva IgG titres in response to meningococcus C polysaccharide vaccine given at 18 months. This study found that a higher relative abundance of Lachnospiraceae at 2 months and Pseudobutyrivibrio, Lachnospira and Roseburia at 12 months and lower relative abundance of Bifidobacteriaceae, Veillonella and Klebsiella at 2 months were associated with higher responses to meningococcus C polysaccharide vaccine (adjusted p < 0.05)24.
Humoral and T-cell response to SARS-COV-2 vaccine were investigated in seven adult studies30,35,45,47,48,49,50. Three studies assessed the humoral response to inactivated SARS-CoV-2 vaccines35,45,47, and five studies to mRNA vaccines (BNT162b2, one also for mRNA-1273)30,35,48,49,50. Two of the mRNA vaccine studies also assessed T-cell responses30,50. A higher relative abundance of several Actynomycetota (Actynomyces, Bifidobacterium adolescentis and B. bifidum)35,49 was associated with a higher vaccine response, while findings for Collinsella aerofaciens were contradictory45,47. The phylum Bacillota was negatively associated with SARS-CoV-2 vaccine responses50, with mixed findings for its classes and orders (higher relative abundance of Clostridia, and lower relative abundance of Eubacteriales among higher responders)45,49,50. There were also inconsistent findings for most of the remaining families and genera: a higher abundance of Lactobacillaceae was associated with higher vaccine responses, but findings for Lachnospiraceae, Clostridiaceae, certain Lactobacillales and Oscillospiraceae were contradictory45,48,49,50. For the Pseudomonadota phylum, a higher relative abundance of Sutterella and Parasutterella excrementihomini, and a lower relative abundance of Succinivibrio and Citrobacter were associated with higher vaccine responses49,50. While a higher relative abundance of the phylum Bacteroidota and the family Rikenellaceae were associated with higher vaccine response, there were contradictory findings for several genus and species within this phylum, including Bacteroides, Parabacteroides, Alistipes and other48,49,50. Finally, a higher relative abundance of Bilophila (a Thermodesulfobacteriota) and a lower abundance of Akkermansiaceae and Akkermansia (Verrucomicrobiotas) were associated with higher SARS-CoV-2 vaccine responses48,50. One study found
留言 (0)