
記住我

The 1678 Health ABC participants included in this study had an average age of 73.6 years, with 52.1% being female and 42.3% self-reporting as black (Table 1). Over the course of an average follow-up period of 11.5 years, there were 371 incident cases of coronary heart disease, 360 incident cases of heart failure, 154 incident cases of stroke, 331 cases of dementia, 356 incident cases of non-skin cancer, 1314 cases of mobility limitation, and 1030 deaths.
Supplemental Tables 2–8 list the senescence biomarkers that were tested for associations with aging-related conditions. In a heat map of correlations between the senescence biomarkers, they were, in general, weakly, or not correlated with each other (Supplemental Figure S1). Correlations with age were weak; however, the baseline age range for Health ABC participants (70–79 years old) was narrow.
Table 2 Summary of the C-statistics (95% CI) for outcomes with models adjusted for clinical covariates and clinical covariates with serum concentrations of senescence biomarkersPatterns of association between senescence biomarkers and disease riskFor almost all associations, higher serum concentrations of senescence biomarkers were associated with an increased risk of the aging outcome. Five biomarkers, GDF15, IL6, MMP1, MMP7, and TNFR2, were significantly associated with all 6 non-cancer aging-related conditions, mortality, mobility limitation, heart failure, coronary heart disease, stroke, and dementia. All of the aging-related conditions were associated with at least several of the biomarkers except cancer which was associated with very few senescence biomarkers. Quantitative details of the associations between all senescence biomarkers and the outcomes are in Supplemental Tables 2–8.
The association between senescence biomarkers and mortality and mobility limitationsTwenty-six of the 35 senescence biomarkers were significantly associated with an increased all-cause mortality. These included GDF15, VEGFA, PARC, MMP2, and TNFR1. Consistent with previous studies that used objective measures of physical function [15], we observed significant associations between 26 biomarkers of cellular senescence and self-reported mobility limitation (Supplemental Table S3).
The association between senescence biomarkers and major age-related diseasesFor cardiovascular diseases, we observed significantly increased risk of incident heart failure (HF) using 20 senescence biomarkers when comparing participants in Q4 to Q1 (Supplemental Table S4). GDF15, IL6, TNFR1, MMP7, and PARC demonstrated the highest HRs for HF. Participants in Q4 compared to Q1 of 14 senescence biomarkers demonstrated significantly increased risk for incident coronary heart disease (CHD) (Supplemental Table S5). Participants in Q4 of GDF15, IL6, Activin A, MCP1 exhibited the highest HRs (all ≥ 1.6) for CHD relative to Q1 participants.
We observed that participants in Q4 of nine senescence biomarkers had increased risk of stroke in the follow-up period compared to participants in Q1 (Supplemental Table S6). Similar to CHD and HF, higher concentrations of GDF15 and IL6, along with TNFR1, Eotaxin, MMP1, and MMP2, conferred the highest HRs for incident stroke.
For dementia, 12 individual senescence biomarkers had significantly greater HRs comparing participants in Q4 with participants in Q1 (Supplemental Table S7). The greatest risk was conferred by the highest quartiles of GDF15, TNFR1, MMP1, MMP7, and µPAR, with participants in Q4 for each biomarker having a HR ≥ 1.6 for incident dementia relative to those in Q1.
Relative to CHD, HF, stroke, and dementia, few senescence biomarkers were associated with incident cancer (Supplemental Table S8). Only Health ABC participants in the highest compared to the lowest quartiles of MMP1, Activin A, and OPN at baseline demonstrated significantly increased risk for cancer during follow-up with HR ≥ 1.4 for MMP1 and OPN.
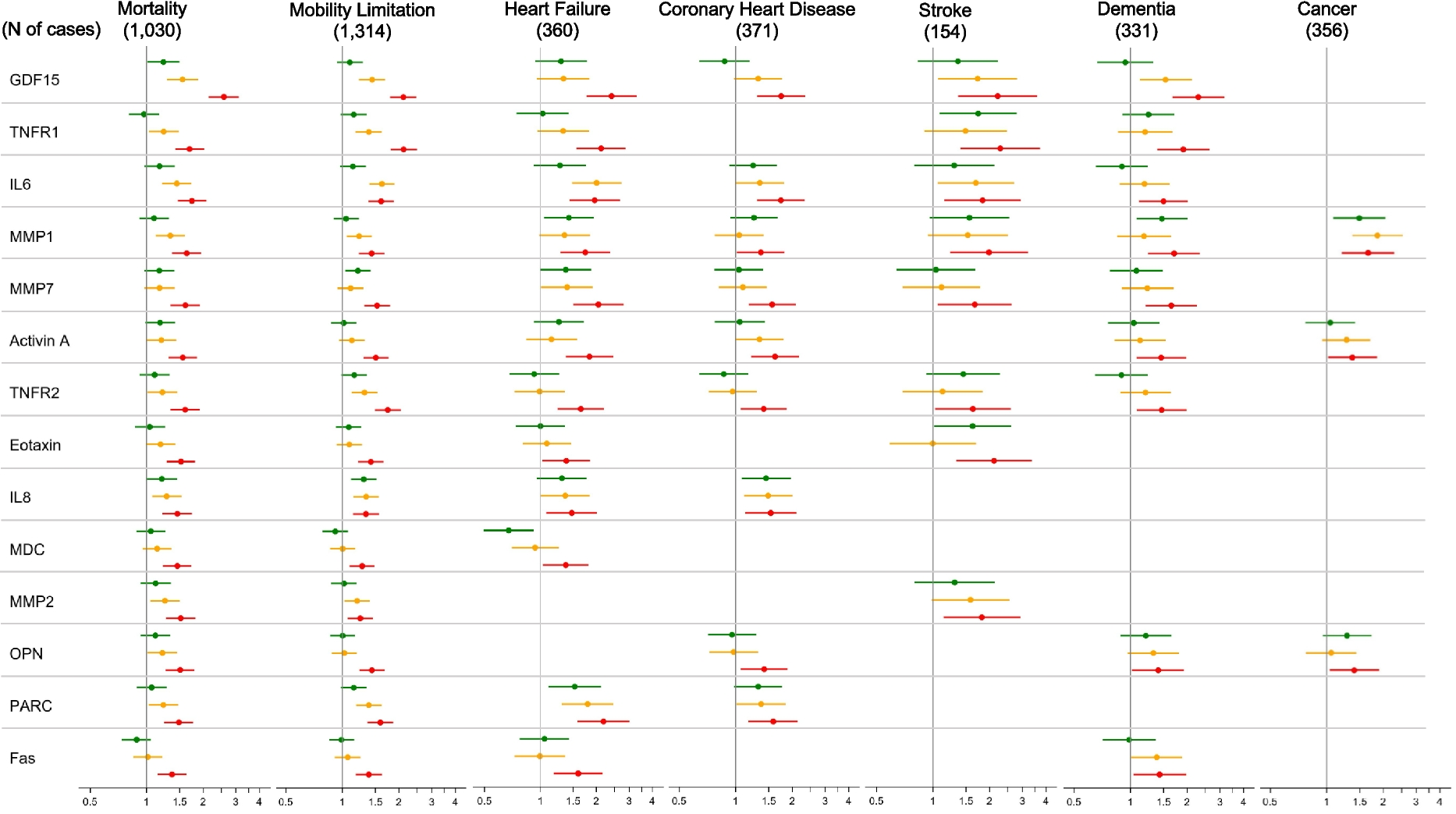
In summary, we noted that the highest levels of eighteen biomarkers were associated with significantly greater HRs for four or more of the six major health outcomes, besides cancer, during the follow-up period (Fig. 1). The highest quartiles of Eotaxin, IL8, OPN, PARC, Fas, MCP1, MPO, STC1, TNFα, and VEGFA were each associated with significantly increased risk for four health outcomes; the highest quartiles of TNFR1, Activin A, and µPAR were each associated with significantly increased risk for five health outcomes, and the highest quartile of GDF15, IL6, MMP1, MMP7, and TNFR2 were associated with significantly increased risk for all six major health outcomes, besides cancer.
Fig. 1

Forest plot of relative hazards for associations between senescence biomarkers and clinical outcomes, adjusted for age, sex, and race using the lowest quartile as the reference group. Only markers with statistically significant associations on the highest quartile are displayed
Senescence biomarkers as predictors of major health outcomes in older adultsTo further examine the added value of senescence biomarkers as predictors of mortality, functional decline, and disease in older adults, we calculated concordance statistics (C-statistics). This approach enabled the comparison of the predictive performance of traditional demographic and clinical variables (i.e., age, sex, and race) with and without the top biomarkers selected for each outcome through LASSO regression.
The addition of senescence biomarkers increased the C-statistics from demographic and clinical variables alone for every outcome (Fig. 2 and Table 2). Addition of the top senescent biomarkers for the condition substantially and significantly increased the C-statistics for mortality, mobility limitation, heart failure, CHD, stroke, and dementia. The addition of the biomarkers made a statistically significant but small difference for cancer. Of note, for mortality, the C-statistics of the demographic and clinical variables alone was 0.61 and addition of the top 7 predictive biomarkers for mortality increased the C-statistics to 0.68 (Table 2). For mobility limitation, the addition of 5 senescence biomarkers increased the C-statistic from 0.58 to 0.66. Addition of GDF15, PARC, and MMP7 increased the C-statistic for heart failure from 0.59 to 0.70. For the occurrence of CHD, the C-statistics for the demographic and clinical variables was 0.59 that increased to 0.65 by the addition of only GDF15 and IL6. Similarly, for stroke the addition of only Eotaxin and IL6 increased the C-statistic from 0.59 to 0.67. Addition of GDF15 and MMP1 modestly increased the C-statistic for dementia from 0.63 to 0.68. The C-statistic for cancer increased little, from 0.61 to 0.64 by the addition of 4 biomarkers, MMP1, Activin A, TRAIL, and uPAR (Table 2). Of note, GDF15 was one of the top biomarkers for all conditions except stroke and cancer.
Fig. 2
C-statistics comparing prediction of outcomes by age, sex, and race (ASR), SASP factors alone, and ASR plus SASP factors. SASP factors, selected by lasso regression, for each comparison are described in Supplemental Table S9–S15
留言 (0)