Fibromyalgia symptomatology extends beyond generalized pain to encompass a spectrum of heterogeneous and nonspecific manifestations. Given the subjective nature and the absence of biomarkers, diagnoses poses a challenge. In the context of SLE, diagnostic is even more complex. The presence of Fibromyalgia complicates both the diagnosis and evaluation of SLE activity, given the overlapping clinical manifestations shared by both conditions. In this study, we investigated the prevalence of Fibromyalgia among Brazilian patients with Systemic Lupus Erythematosus (SLE) and its impact on their quality of life. Employing both the 1990 and the revised 2010/2011 ACR criteria enhances diagnostic accuracy and ensures a comprehensive assessment of Fibromyalgia [25]. This research addresses a significant gap in understanding comorbidities in this population, highlighting the substantial burden that Fibromyalgia imposes on the quality of life of SLE patients.
Fibromyalgia was identified in 19.1% (21) of the SLE patients included in our study. This prevalence aligns with observations from previous studies, which reported Fibromyalgia frequencies among SLE patients hovering around 22% [9, 11, 12]. Contrasting with prior Brazilian data which reported a 12% prevalence of Fibromyalgia in SLE patients, this current investigation unveiled a notably higher prevalence. The earlier Brazilian study examined a smaller patient sample, segregating them into three categories: Fibromyalgia, SLE, and Fibromyalgia + SLE. Their findings indicated that while Fibromyalgia did not exacerbate SLE activity rates, it notably impaired the quality of life in SLE patients [13]. No other comparable studies assessing the Brazilian population are documented in the literature.
When comparing the sociodemographic characteristics of SLE patients with and without Fibromyalgia in our sample, notable differences emerge. The average age of SLE patients without Fibromyalgia is 42.9 years (± 12.52), while those with Fibromyalgia are slightly older, averaging 45.6 years (± 9.76). In terms of gender, the group without Fibromyalgia consists of 94.1% females and 5.9% males, while the group with Fibromyalgia is entirely female. Education levels are similar between the groups; however, a higher percentage of patients without fibromyalgia are employed (34.1%), compared to only 19.1% in the fibromyalgia group. These differences underscore the negative social impact of fibromyalgia on patients with lupus, particularly in terms of employment and daily functioning.
In comparing the two groups based on the SLICC-2012 criteria for lupus, most clinical criteria were found to be similar. However, the group with fibromyalgia exhibited a higher prevalence of acute cutaneous manifestations, such as malar rash, with 81% (17 patients) compared to 75.6% (65 patients) in the lupus-only group. Additionally, alopecia was more common in Group 2, affecting 71.4% (15 patients) versus 60.5% (52 patients) in Group 1. Both groups showed similar rates of chronic cutaneous involvement, arthritis, renal issues, serositis, and neurological manifestations. Immunological profiles were also comparable. In Group 1, 95.3% (82 patients) had positive antinuclear antibodies (ANA), with 17.4% (15 patients) showing anti-DNA antibodies and 11.6% (10 patients) positive for Anti-SM. Group 2 had 95.2% (20 patients) testing positive for ANA, 14.3% (3 patients) for anti-DNA and 19% (4 patients) for anti-SM.
A very recent study [26] yielded results consistent with our findings. The authors compared the clinical phenotype-laboratory characteristics between lupus patients with and without Fibromyalgia. No differences were noted between the groups, except for a higher incidence of malar rash and active arthritis in Fibromyalgia patients, despite similar autoantibody profiles. The study also found no correlation between fibromyalgia and disease activity, as assessed by the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2k) [27]. This finding aligns with numerous previous studies [5, 11, 13, 18, 28, 29].
Fibromyalgia diagnosis relies on criteria outlined by the American College of Rheumatology (ACR). The 1990 criteria primarily require diffuse pain presence (above and below the waist, right and left sides, and axial) and tender point examination, with at least 11 of the 18 sites being tender [20]. In our study, 15.8% (17) of patients exhibited 11 or more tender points, slightly lower than another study’s findings, which concluded that 17.3% of SLE patients had 11 or more tender points. The American study further revealed worsened health status, as assessed using the Health Assessment Questionnaire, in SLE patients with a higher number of tender points, even without Fibromyalgia diagnoses [30].
Given Fibromyalgia’s multifactorial nature and symptomatic heterogeneity, questionnaires are indispensable for objectively assessing affected patients’ quality of life. The Fibromyalgia Impact Questionnaire (FIQ) is widely employed for this purpose due to its simplicity and effectiveness. This tool gauges functional capacity, employment status, psychological disorders, and physical symptoms, proving reliable in evaluating Fibromyalgia therapeutic efficacy [31]. First published in 1991 and subsequently revised in 1997 and 2002, the FIQ was culturally adapted for the Brazilian population and validated in 2006 [24]. Among Fibromyalgia patients assessed with the FIQ in our study, pain and fatigue emerged as the most detrimental to quality of life, corroborating findings from a prior Brazilian study [13].
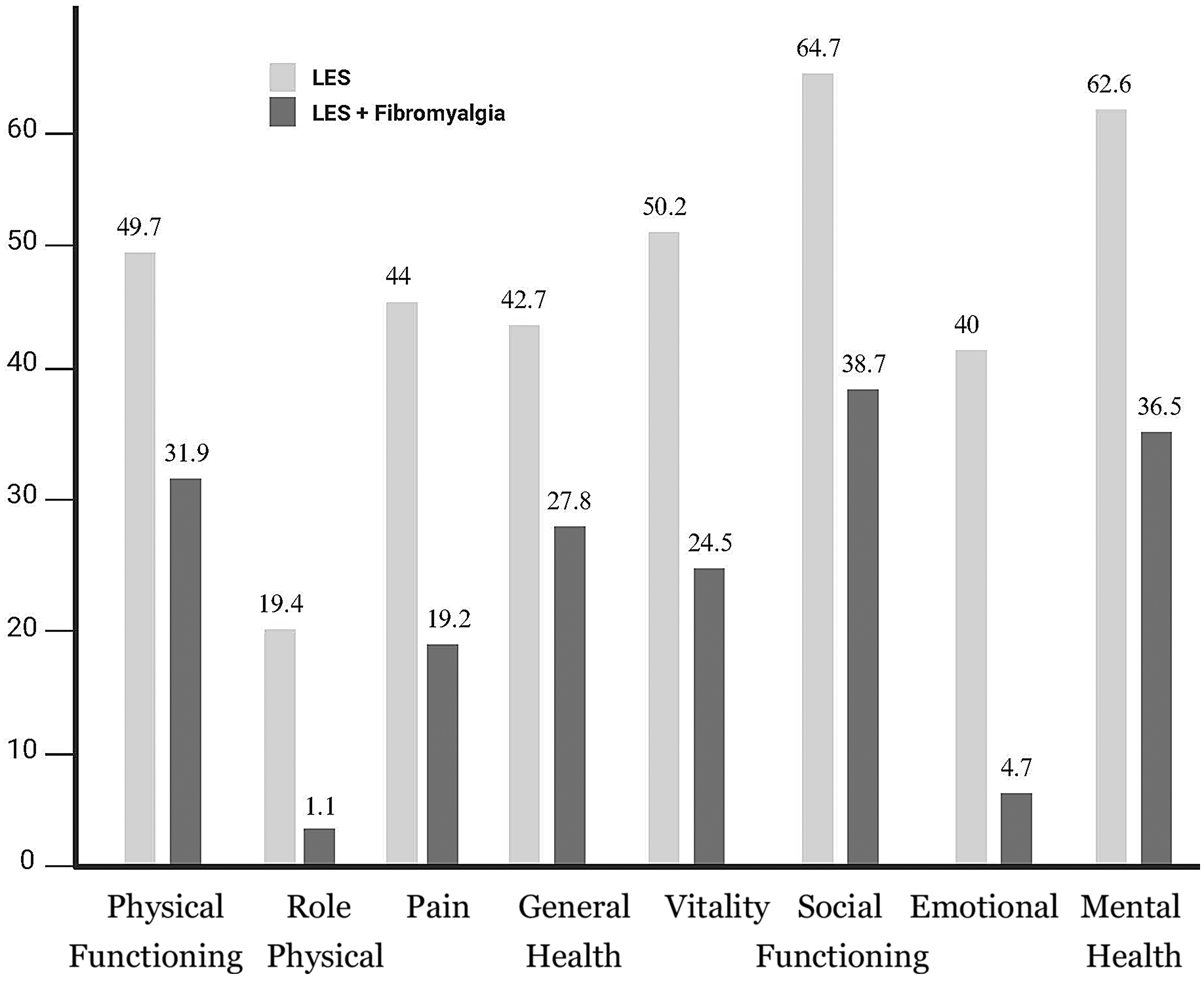
The SF-36 questionnaire assesses quality of life across eight domains: functional capacity, physical aspects, pain, general health status, vitality, social aspects, emotional aspects, and mental health. Application of the SF-36 in the present study revealed lower scores across all eight domains among SLE patients with Fibromyalgia compared to those without. This pronounced negative impact of Fibromyalgia on lupus patients’ quality of life echoes findings from previous studies using the same instrument [29, 32]. These data underscore the criticality of early Fibromyalgia diagnosis and appropriate therapeutic management to enhance SLE patient well-being.
Studies evaluating Fibromyalgia’s impact on SLE patients’ quality of life using alternative tools have also demonstrated the syndrome’s adverse effects. A 2009 Spanish study uncovered an association between Fibromyalgia and anxious and depressive psychiatric symptoms. Utilizing the Short Form 12 questionnaire (SF-12), the study reported lower scores in both the physical and mental components among Fibromyalgia- afflicted individuals [33, 34]. Valencia-Flores et al. [35] evaluated Fibromyalgia and SLE patients’ functional statuses using the Health Assessment Questionnaire Disability Index (HAQ-DI), validated for their demographic. Fibromyalgia patients exhibited higher disability rates, alongside increased occurrences of sleep disturbances, fatigue, and depression.
The 2019 European Alliance of Associations for Rheumatology (EULAR) recommendations for SLE management include enhancing Health-Related Quality of Life (HRQoL) as a treatment objective [36]. While remission or low disease activity are ideal therapeutic goals, conflicting data regarding their impact on HRQoL improvement exist in the literature. A recent study highlights Fibromyalgia as a contributor to discordance between SLE patients’ self-perceived health statuses and physician-reported disease activity measures [37]. These findings emphasize the necessity of early Fibromyalgia diagnosis and proper comorbidity management to foster SLE patient well-being.
The study faced several limitations. Despite employing questionnaires validated for the Brazilian population, several patients experienced challenges in understanding the questionnaires, which may have affected their responses. Additionally, we did not evaluate disease activity in SLE using the SLEDAI-2k as a variable in our study, nor did we assess the SLICC/ACR Damage Index (SDI). Another significant limitation was the absence of a healthy control group and a group consisting solely of patients with Fibromyalgia.








留言 (0)