A framework proposed for incorporating capacity constraints into economic evaluations is summarised in Table 1, and methodological considerations for each of the steps are described in detail in the subsections below. This framework is designed with a focus on high-income settings, reflecting the specific resource allocation challenges and health system structures typical of these environments. The framework proposed in this manuscript was developed on the basis of the collective experience and expertise of the authors in operations research and health economics. It aims to provide guidance for integrating resource constraints into economic evaluations, recognising that this is an emerging and evolving field. The iterative development process involved two initial workshops with all authors, where the majority attended in person and the rest participated online. Key perspectives and the manuscript’s foundation were agreed upon during these sessions. This was followed by several rounds of offline reviews, with additional comments incorporated after consensus was reached through a collaborative exchange of authors ideas using various communication tools, including document comments and emails, ensuring a comprehensive consideration of various perspectives and refinements.
Table 1 Framework for incorporating constraints in economic evaluations [4, 10,11,12,13]It is important to emphasise that the steps can be performed in a different sequence; the process of resource modelling is iterative rather than a strictly sequential set of steps.
In situations where the resource constraints are not estimated explicitly, it is also possible to use a subset of steps in the framework. By skipping steps 4 and 5, the impact of the constraints on costs and QALYs can be assumed directly in steps 6 and 7 without modelling the constraints or their impact on the healthcare system. Similarly, qualitative approaches can involve conducting steps 1, 2 and 9 (i.e. skipping steps 3–8) where the impact of constraints on the healthcare system is described qualitatively.
This framework is designed for situations where the resource constraints are estimated explicitly (i.e. those outlined earlier as quantitative approaches). It further assumes that the typical economic evaluation considerations, including treatment alternatives, population, outcomes and perspective, are predefined. Thus, it solely focusses on the additional factors required for integrating resource constraints into economic models. In cases where data are not available in published literature, expert input should be considered to ensure that the estimations and assumptions are accurate.
4.1 Step 1: Choosing the Setting (Local Versus National)
The selection of the setting for estimating constraints, whether at a national or local organisation level, should depend on the targeted decision-maker or budget holder in combination with the feasibility of estimating the resource constraints’ impact at local, regional or national levels.
When resource constraints are at a national level (e.g. capacity for cancer screening), modelling can be done at a national level, and data can be generalised for local settings. A local approach can provide more robust results that are relevant to that specific healthcare setting and can be verified by comparison with the data in that setting. However, such results may not be easily generalised to the national level, and their usability for a traditional national HTA will be limited. A nationwide approach might involve identifying and developing models for key representative setting types (e.g. small hospitals, mid-sized hospitals, large hospitals). If the patient pathway is similar between settings and the differences can be captured as parameters (e.g. the number of beds), a single, generic model can be developed, which can be amended to represent the different settings. It is important to note that selecting the base case is necessary, and expert opinion should drive this selection.
4.2 Step 2: Identifying and Selecting the Constraints
Healthcare systems involve a wide array of resources, each with their own potential for constraints that can affect overall efficiency and effectiveness. The challenge lies in distinguishing which of these constraints should be quantitatively estimated and which can be managed qualitatively.
This process involves two stages: first, the identification of potential constraints in the healthcare system; and second, the careful selection of those constraints that are most likely to influence the cost-effectiveness of any given intervention.
To identify resource constraints in healthcare systems, it can be beneficial to apply implementation science frameworks, such as the Consolidated Framework for Implementation Research [30]. These frameworks offer a structured approach to analysing various factors influencing the implementation of healthcare interventions, facilitating a comprehensive identification of potential resource constraints.
A large number of potential constraints are likely to be identified in an initial search. Because of modelling limitations, it is unlikely to be possible to model the impact of every constraint, and many of the constraints are unlikely to have a meaningful impact and do not need to be estimated. It has been suggested that the modelling of constraints could be useful when (1) a new technology needs considerable additional resources compared with the current situation; (2) the new technology is reliant on occupied resources, or the occupied resources related to the new technology are specialised; (3) specific resources are known to be in short supply; or (4) the new technology has a positive effect on already existing queues [16].
To narrow down the number of constraints to be modelled, a process of constraint selection must be undertaken. One potential approach for resource constraint selection is scenario drafting, which is a method used to create and analyse various plausible future scenarios, especially in situations with high uncertainty, to aid in decision-making and strategic planning [31].
In both stages—identification and selection of resource constraints—it is important to seek opinions from clinical experts, as well as from the professionals responsible for the running of the services, to understand and validate the key resource constraints involved in an intervention. Methods such as the Delphi technique, structured interviews, and nominal group techniques can be used to effectively gather and synthetise experts’ opinion. Attention should be directed to resources facing constraints that are not transitory in nature but will span an extended period (at least the medium term).
As previously mentioned, sometimes multiple resources can be combined into a single unit of resource constraint. For example, a clinic visit can be used as a resource constraint, encompassing various resources, such as doctors, nurses, space and diagnostic services.
4.3 Step 3: Choice of Modelling Technique
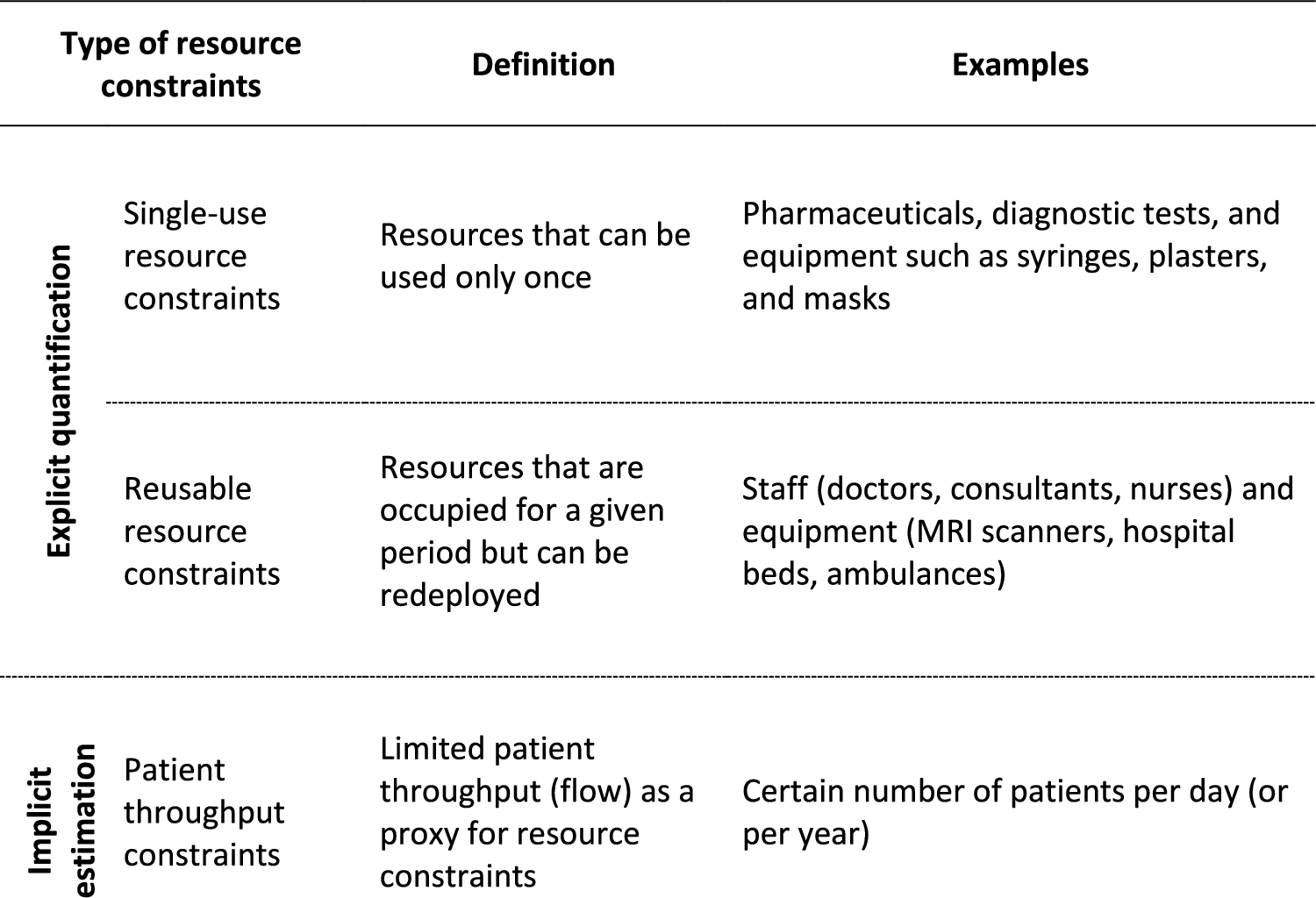
The choice of modelling technique is linked to the type of resource constraints. For single-use and patient throughput resource constraints, it is possible to link the health states to resources using static traditional economic evaluations cohort modelling techniques (such as semi-Markov models and decision trees) to estimate the overall resources required and understand whether there is enough capacity. Advanced simulation techniques, such as discrete event simulation or system dynamics modelling, can also be used for these constraints, but the simplest model possible for each situation should be used where possible.
For reusable resources, advanced simulation techniques are required. These techniques help comprehend resource availability fluctuations and estimate whether there is adequate capacity to accommodate the rate of demand (e.g. patient arrival rate) and occupancy duration (e.g. hospital length of stay) [1]. Discrete event simulation models are more flexible than cohort models because they allow for the modelling of alternative patient pathways or management of waiting lists subject to pre-defined characteristics while providing more detailed results (e.g. queue size/waiting time) [32]. Additionally, SDM can be used to identify and understand constraints within the healthcare system. SDM explores interactions and feedback loops within the system, helping to uncover how constraints in one area may impact others. This approach is useful for identifying constraints that may not be immediately apparent and understanding their potential long-term effects on system performance.
4.4 Step 4: Selecting Data for the Constraints
For single-use resources and patient throughput, the constraints are included in the model directly. Reusable resources (e.g. beds) will require additional data, such as availability (e.g. schedules/shift times), patient arrival rate, and time of occupancy (e.g. length of stay). For resources with multiple uses (e.g. magnetic resonance imaging scanners), the use of the resource in ways unrelated to the modelled intervention may also need to be considered.
Published literature, if available, can be used as a data source but needs to be checked for face validity. If no data are available, primary research or expert opinion could be used to parameterise the constraints. For patient throughput constraints, it is important to carefully consider the data and check the rationale behind the assumptions to ensure that throughput used has face validity.
4.5 Step 5: Estimating process impacts on the healthcare system
As described earlier (Fig. 2 Taxonomy of the potential impact of constraints), the impact of the constraints manifests as an effect on the production process of the healthcare system, such as fewer patients receiving the intervention, increased delays in treatment or longer queues/higher waiting times. For single-use resource constraints or patient throughput constraints, these service impacts can be modelled in the short or long term. However, for reusable resource constraints, these process impacts are always short term; potential organisational changes, treatment pathway changes or corrective actions cause uncertainty in predicting long-term process impacts.
In addition, it is possible to directly model the impact of constraints on costs and QALYs using assumptions (e.g. changing the cost or changing the quality-of-life gains because of uptake); however, this option does not consider the resource constraints’ impact on healthcare system operations.
4.6 Step 6: Estimating the Impact on Quality-Adjusted Life Years
The impact of resource constraints on QALYs can be estimated by modelling their effect on the production process of the healthcare system. As previously mentioned, in some situations the impact of the constraints on QALYs can be assumed directly without modelling the impact of the constraints on the healthcare system.
The impact on QALYs depends on the type of process impact of the constraints. For reusable resource constraints, the impact of treatment delay can be estimated as reduced life expectancy and/or lost utility on the basis of the clinical condition. However, single-use constraints or patient throughput constraints can place a limit on the number of patients treated with the intervention, which can be estimated as a net loss in the NMB. This overlaps somewhat with the concepts around the value of implementation [33].
4.7 Step 7: Estimating the Impact on Costs
The impact of constraints on costs, sometimes reflected in charges or distorted prices, depends on the type of production process impact the constraints have and the available corrective actions.
Although estimating the cost and impacts of constraints using general equilibrium theory or opportunity costs is a complex task requiring detailed data and extensive time for analysis, it should not be dismissed as unfeasible. Indeed, the challenges involved, such as the need for granular data and the difficulty of estimating opportunity costs, make it a particularly intriguing subject for in-depth study. See Section 6.3 for further discussion about this issue.
Estimating the opportunity cost is also challenging because assumptions need to be made about the use of free resources. For example, if there is a day bed free, we need to make assumptions about the likelihood that it would be used by a sick patient or by a recovered patient who could not travel home that day.
As such, the cost impacts can be estimated by considering the unit costs of resources and the liquidity of the resources (e.g. assuming patients with delayed treatment can be transferred to premium out-of-hours/outsourced clinics, which results in increased costs). Cost impacts of other corrective actions, such as an increase in capacity, could be estimated using a bottom-up approach or by approximation using unit costs, along with assumptions about any increased costs.
In some situations, the impact of resource constraints on costs can be assumed directly (e.g. changing the cost) without modelling the impact of the constraints on the healthcare system.
4.8 Step 8: Sensitivity Analyses and Model Validation
Standard tools used in cost-effectiveness models to characterise parametric uncertainty (such as deterministic or probabilistic sensitivity analysis [PSA] or scenario analyses) can also be used to understand the uncertainty around the impact of constraints. For example, assessing the impact of small increases in constraints would be useful.
For model validation, it is first important to compare the results of modelling without constraints with any similar models to ensure that the model has face validity. Models with constraints can be validated by reducing the inputted constraints to zero and comparing them with the model without constraints.
4.9 Step 9: Incorporation into Economic Evaluations
Methodologically, there are different ways in which constraints could be incorporated into economic evaluations.
One option is to model the effect of constraints on costs and QALYs quantitatively and incorporate them directly into the estimation of the cost-effectiveness of an intervention (e.g. ICER). This option would provide information regarding the impact of constraints on the outcomes of an intervention. Estimating the outcomes of the intervention (e.g. costs, QALYs) without modelling the constraints might introduce more uncertainty into the results because of the assumptions required, which can reduce the robustness of the information provided.
In situations where the constraints impact the ICER in a less obvious way, such as when modelling patient throughput constraints, it is important to consider outcomes other than ICER, such as the population-level NMB or population-level ICER.
Alternatively, in situations in which the resource constraints are not estimated explicitly, thus not contributing to the economic assessment, the impact of constraints on the healthcare system outcomes (health and costs) can be described qualitatively.







留言 (0)