
記住我





This objective was investigated by an economic modelling approach that evaluated the impact of improved reuse behavior on outcomes related to insulin consumption, hypoglycemic events and diabetes-related complications. The comparison of a situation of insulin injection without PN provisioning with the situation where PwD are provided with PNs and targeted educational support enabled us to calculate savings in health care expenditures. The initiation of model development and population was guided by a narrative literature search to identify the clinical benefits of PN reuse rate reduction. Belgium represents a rare exception in Europe as one of the few countries where insulin PN are not reimbursed. Due to the lack of data on this aspect, input from Belgian clinical experts was deemed essential to further guide this economic evaluation.
A validation process was established, consisting of three sequential stages. Belgian experts in diabetes clinical management and health economics were consulted individually to provide relevant inputs and insights. After completing the initial version of the model, a technical briefing document and a structured questionnaire were sent to all experts. This material outlined the current efforts and asked the experts whether they agreed with the model’s inputs and assumptions. If any expert disagreed with a specific assumption or parameter value, they were given the opportunity to suggest an alternative. In the next stage, an in-person consensus meeting with six clinical experts was held to discuss the survey results and gather additional recommendations. A final report was then prepared, summarizing the consensus on the model’s configuration and parameters, which was reviewed and approved by all experts. In cases where the clinical experts did not agree with certain parameter estimates from the initial model configuration, a midpoint value was calculated and used as the input for the base-case configuration. The following sections provide more details on the study’s evaluation, including the sources, selection process and population of model parameters and assumptions (Tables 1, 2).
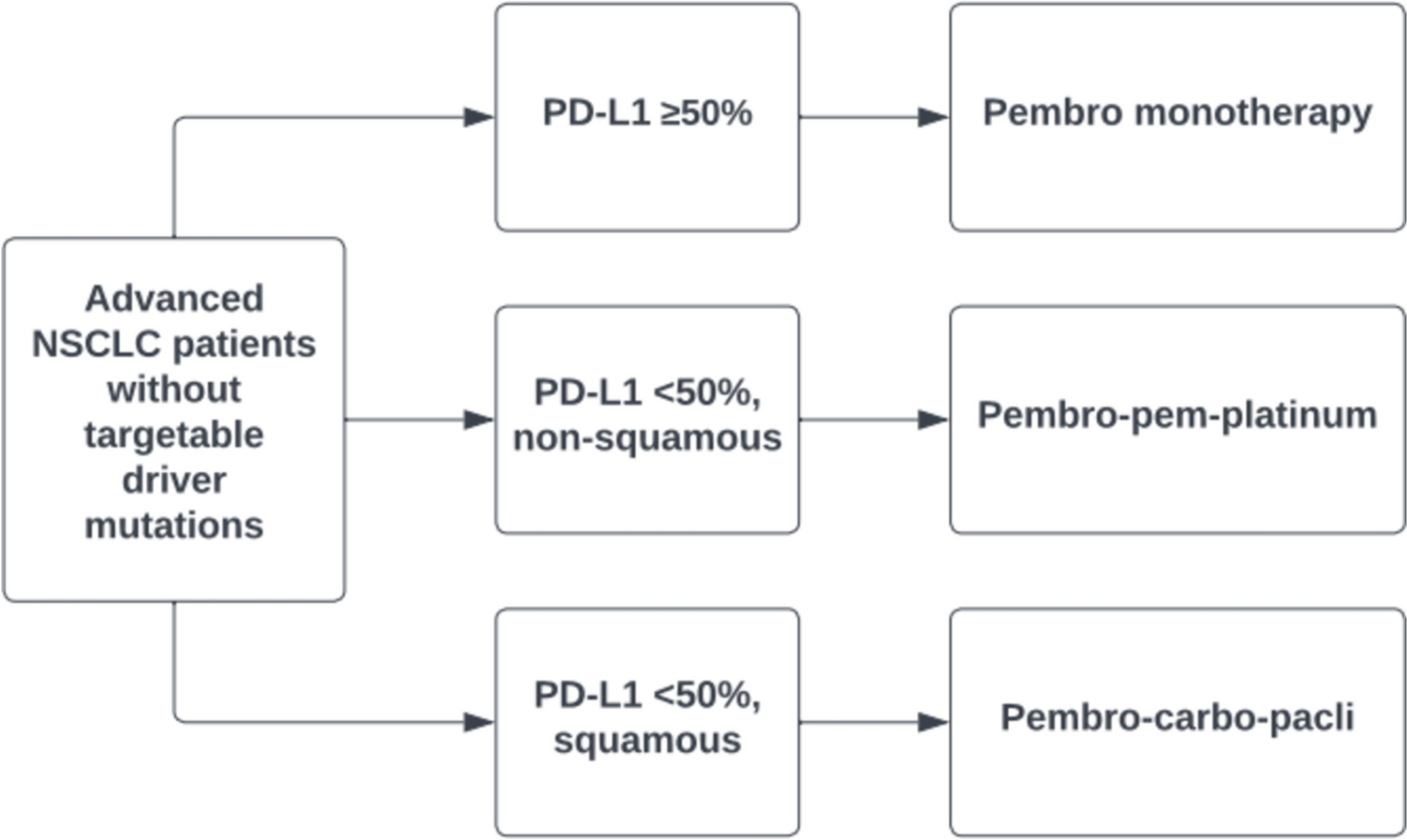
Table 1 Model input parameters and sourceTable 2 Cost input parameters and source2.2 Model StructureThe analytical modelling framework was developed in the programming language R and captures dependencies between PN reuse and LH status as well as between LH status and health care expenditures. The structure of the implemented model is depicted in Fig. 1 and illustrates the flow of patients. [A] The model starts with a set of structural parameters and defined subpopulations. [B] The starting patient population is then divided into different groups based on usage frequency of a single insulin PN. [C] Patients within each group are assigned an LH positive (LH+) or LH negative (LH−) status, with the prevalence of LH+ and LH− in each group proportional to the increased risk of LH associated with increased PN reuse. A negative LH status refers to regression (a reduction in prevalence or size) of existing LH nodules, mitigation of incident LH development, as well as the practice of not systematically injecting into LH nodules. A positive status refers to the persistence of inadequate IIT, existing nodules or the development of new LH nodules. [D] Patients’ LH status is linked to a value for insulin TDD, the number of hypoglycemic episodes per year and the risk of long-term complications (as a function of HbA1c). The time horizon of the analysis was set at 1 and 5 years, reflecting time windows used in Belgium for economic modelling of budgetary impact in the context of reimbursement submissions.
Fig. 1
Model structure and the different building blocks. Letters denote the different building blocks as discussed in the Methods section. Flow of PwD across the model is shown from sections A to C, and the outcomes considered as output in section D. LH lipohypertrophy, TDD total daily dose
2.3 Model Input Parameters2.3.1 Patient PopulationThe target population includes all PwD with T1DM and T2DM in Belgium that require insulin injections using PN. We defined three subpopulations depending on diabetes type and the care system in Belgium in which people were enrolled. In Belgium, education and self-monitoring materials are provided through the Diabetes Convention or the Diabetes Care Pathway. The diabetes convention is aimed at people with type 1 (subpopulation 1) or type 2 (subpopulation 2) diabetes treated with complex insulin therapy (three or more daily injections). The care pathway is for people with type 2 diabetes who are treated with one or two daily injections (subpopulation 3). Population numbers were obtained from the IKED study (Audit 11), a quality assurance database of Diabetes Convention patients [17] and from Farmanet, a public database of pharmacies (RIZIV). Subpopulation 1 included 33,035 PwD in Diabetes Convention, subpopulation 2 included 74,752 PwD in Diabetes Convention and subpopulation 3 included 62,609 PwD in Diabetes Care Pathway (Table 1). The average number of injections for each patient population was calculated as per the LIMO [4] and IKED studies [17] for the Diabetes Convention, and suggested by clinical experts for the Diabetes Care Pathway.
2.3.2 Frequency of PN ReuseAn estimate of reuse prevalence in the Belgian target population was informed by the Worldwide Injection Technique Questionnaire (ITQ) and LIMO studies [4, 16] (Table S1, see electronic supplementary material [ESM]). We further grouped the reusing population into four categories according to frequency of PN replacement. The proportion of PwD across single use or the different reuse categories was based on the LIMO study [4].
2.3.3 Risk for LipohypertrophyImpaired adherence to injection guidelines has been associated with an increased risk for LH+ status. The increasing risks for LH+ for each of the different reuse categories and an overall risk ratio for reuse, compared with single use, were obtained from Blanco et al. [18] (Table 3). These risk ratios were used to quantify the prevalence of LH among the different reuse categories, using the prevalence of LH+ in single use PwD.
Table 3 Risk ratio and LH prevalenceWhile the current LH+ prevalence in single-use PwD is unknown for Belgium, an LH+ prevalence of 63% was reported among a patient population frequently re-using PNs [4]. From a back-calculation based on the overall risk ratio of 1.34 (Table 3), an estimate of 47% can be obtained for the prevalence of LH+ in single-use PwD in Belgium. Clinical experts did not agree with this estimate and selected a prevalence estimate of 27% as the lowest value from a range of options. As a result, a midpoint value of 37% for the prevalence of LH+ in the single-use population was included in the base-case analysis (Table 1).
2.3.4 InsulinResearch shows that LH often leads to an increase in insulin TDD, although the magnitude of the observed increase varied across studies, up to 35% (Table S3, see ESM) [4, 11, 15, 18,19,20]. Guided by clinical expert opinion, a TDD difference of 10 IU per LH status was chosen to reflect the consensus among clinical experts and the distribution of values collected. The cost of one unit of insulin was obtained from a weighted average of the cost of insulins provided in Belgium in 2022 (Table S3, see ESM).
2.3.5 Hypoglycemic EventsThis study only took ‘severe’ and hypoglycemic events ‘requiring hospitalization’ into consideration. Severe hypoglycemic events were defined as events leading to unconsciousness, requiring assistance of a third person, often associated with blood glucose levels below a predefined threshold [21, 22]. Because of a lack of standardized definitions, this threshold value can vary across studies [23]. Estimates on the number of events per year were collected to calculate the burden of hypoglycemic events depending on the LH status of PwD.
The number of severe events per year per person for T1DM was obtained from the Belgian FUTURE study [24], which reported estimates before and after the use of continuous glucose monitoring (CGM) (Table S4, see ESM). The rate of severe events for PwD with T2DM was calculated using the T1DM/T2DM ratio from Tzogiou et al. [25]. The number of events requiring hospitalization for PwD with T1DM and T2DM was extracted from the RELIEF study [26], which reported event rates before and after use of CGM.
For each DM type, we calculated the number of hypoglycemic events per patient per year by using the before-CGM and after-CGM rates balanced for the proportion of patients on CGM in each group (CGM-uptake weighted averages) [17]. The obtained numbers of hypoglycemic events were further rescaled towards LH+ and LH− status to reflect an increased risk of experiencing a hypoglycemic event if LH+ [9] (Table S5, see ESM).
Costs associated with severe hypoglycemic events for PwD with T1DM and T2DM were derived from de Groot et al. [27], who assessed per-patient costs of hypoglycemia in 2016 among PwD with T1DM and T2DM in The Netherlands. Costs associated with an event requiring hospitalization for PwD with T1DM were reported in the RESCUE study [28] for 2018, while the respective cost for PwD with T2DM was estimated using the T1DM/T2DM cost ratio of severe events.
2.3.6 Long-Term ComplicationsThe prevalence of the different types of chronic clinical complications among Belgian Diabetes Convention PwD with T1DM and T2DM was obtained from Lavens [29] (Table 1, Table S6 in the ESM). The UK Prospective Diabetes Study (UKPDS) has shown that improved glycemic control over 10 years can reduce vascular complications of PwD with T2DM, quantifying the relative risk reduction for long-term complications with each 1.0% decrease in HbA1c [30, 31]. Converted to 1-year and 5-year probabilities, these HbA1c-driven risk reductions were applied for both T1DM and T2DM populations in the model. For the difference in HbA1c between LH status, we used the value of improvement reported for a subset of patients with non-optimal metabolic control in the LIMO study [4] (Table S7, see ESM). For each category of long-term complications, a weighted mean cost per patient was calculated from the related APR-DGR for 2021 [32].
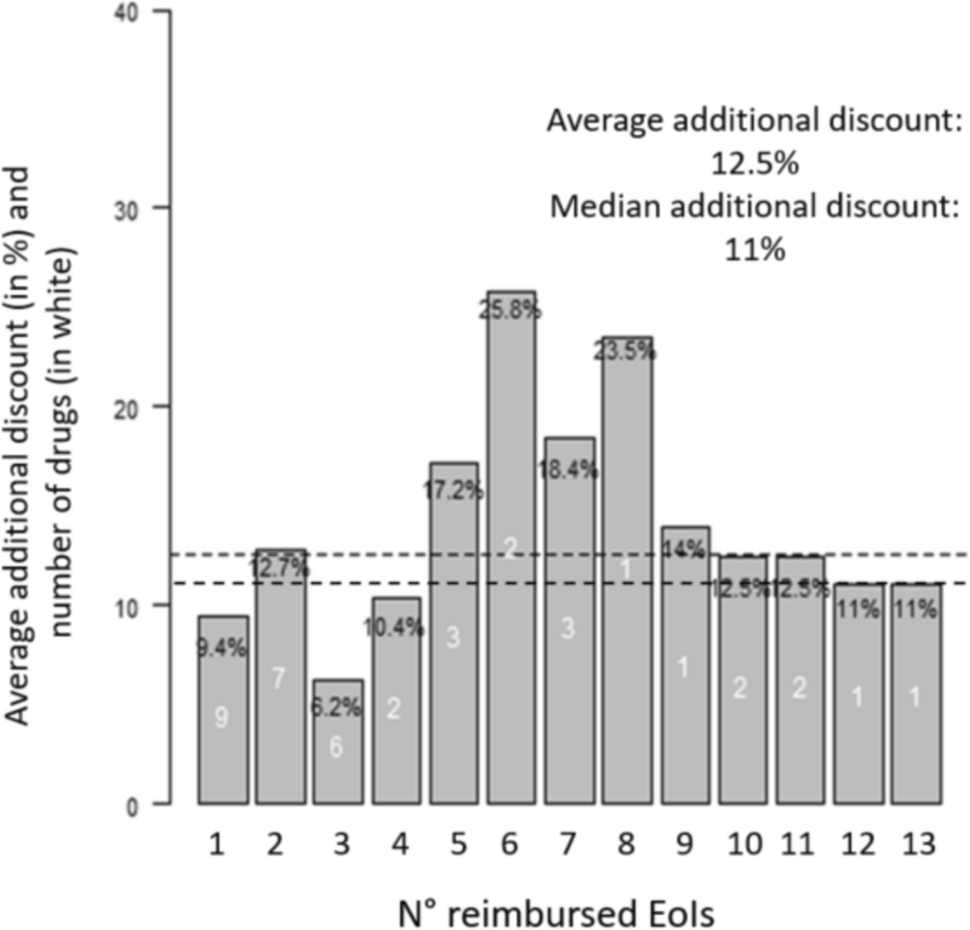
2.3.7 Impact of the InterventionThe effect of free PN provisioning complemented with targeted educational support on single PN use was modelled to cause a shift in reuse distribution (Table S2, see ESM). A reduction in reuse prevalence from 90% to almost 20% was reported following the intervention in the LIMO study [4], while clinical experts indicated that a reduction to 50% was more appropriate according to their expertise. Following the mid-point strategy, a reduction in reuse prevalence from 90% to 35% was implemented, implying a shift towards single use behavior for 55% of PwD (Table 4). Furthermore, the remaining PwD reusing PN largely shifted towards lower reuse frequency (Fig. 2).
Table 4 Patient population and LH prevalence before and after the intervention after 5 yearsFig. 2
Population distribution across reuse categories. For each category denoting the number of times a single PN is used, the proportion (%) of the population is shown before and after the intervention
Importantly, due to the model structure, a change towards a LH− status was only predicted for a subset of persons who improved IIT, with the size of this subset being dependent on the difference in LH+ prevalence between single using and reusing populations. Moreover, the impact on model outcomes was introduced in a gradual and delayed manner. The time window and magnitude of LH status improvement was calculated from literature and modelled to affect, every 6 months, 65% of the respective PwD subset (Table S8, see ESM). This estimate corresponds to the proportion of patients in the ISTERP-2 control group who experienced full or partial remission of LH after 6 months, with this group being considered representative of the current situation in Belgium [5]. The model was run in absence and in presence of the intervention, with a time horizon of 5 years to calculate the difference in economic burden for the PwD population in this study. No discounting was applied for cost or effects.
2.4 Scenario and Sensitivity AnalysesA deterministic sensitivity analysis of the base-case configuration by varying parameter values by 20% was performed to assess the robustness of the model and factors impacting the model’s outcomes. The model’s base-case configuration was established using parameter values that reflected a consensus between estimates from the literature search and the opinions of clinical experts on the Delphi panel and parameters for which a midpoint value was selected in absence of consensus. To explore the impact of the source for these latter parameters, two scenario analyses were conducted, one using only input values from the literature and the other using the input values as provided by the clinical experts. A third and fourth scenario analysis was conducted to evaluate to what extent the magnitude of CGM uptake had an effect on the model outcomes. While the base-case analysis reflected the current clinical practice in Belgium, with varying levels of CGM use across the patient populations, the scenario analyses considered scenarios where CGM was not yet part of diabetes management or where it was well established with all PwD using CGM.
留言 (0)