2.1 Study Design
This analysis was based on data from the ongoing multicenter implementation study Dementia Care Management: Implementation into different Care Settings (DCM:IMPact), which aims to translate the proven effective and cost-effective DelpHi-Intervention into various healthcare settings (e.g., physician networks, day care, or community health center) from different sectors to identify the setting with the highest needs, lowest implementation barriers and best achievable effects to subsequently foster a large scale, sustainable, and cross-sectoral translation of cDCM [15, 32]. The cDCM intervention is conducted by dementia-specific qualified nurses (dementia care manager) and was developed and evaluated within the DelpHi-MV trial [15, 17]. The detailed study design and intervention have been described elsewhere [17]. The intervention implementation costs are described in Supplementary Table 1.
The implementation is based on the framework of Mendel et al. [33], which focuses on the dissemination and implementation of interventions in mental health services research, starting the dissemination process with contextual factors, such as structures, resources, and policies that should be reflected in the actual implementation process. The subsequent outcome evaluation should produce the need for adjustment on the intervention level and influence the contextual factors, with the latter in particular determining the most crucial aspect of dissemination. Accordingly, the DCM:IMPact study follows two steps: the individual settings are first examined separately (medical versus nursing care), and on the basis of these findings, cDCM will be enhanced to a cross-sectoral approach to overcome the challenges arising from German healthcare’s legal, organizational, and financial fragmentation as contextual factors [33].
So far, one physician network (comprising n = 22 participating practices), representing medical care funded by health insurances and two day care facilities, representing nursing care funded by long-term care insurances, were completed in 2023. The participating healthcare providers were located in a rural area in north-eastern Germany. Each setting employed one dementia care manager. In total, n = 136 eligible patients met the following criteria: aged ≥ 70 years old, living at home, DemTect < 9 [34], or formal dementia diagnoses according to the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10) [35], were informed about the study by the respective healthcare professionals, and provided informed consent approved by the ethical committee of the Chamber of Physicians of Mecklenburg-Western Pomerania—registry number: BB01/2019.
A comprehensive, standardized, computer-assisted face-to-face interview was conducted by the respective dementia care manager at the participants’ homes at baseline (t0) and 6 months after (t1), and was completed by n = 100 PwD. Patients who dropped out of the study were statistically significantly less likely to enroll in DCC [odds ratio (OR) = 0.06; 95% confidence interval (CI) 0.01–0.26; p < 0.001) and were less likely to have received a formal dementia diagnosis (OR = 0.20; 95% CI 0.07–0.58; p = 0.003). A detailed drop-out analysis is shown in Supplementary Table 2.
2.2 Data2.2.1 Sociodemographic and Clinical Characteristics
The following demographic data and clinical variables were assessed: age, sex, living situation, cognitive impairment according to the mini-mental state examination (MMSE) [36]; deficits in daily living activities according to the Bayer activities of daily living scale (B-ADL) [37]; depressive symptoms according to the geriatric depression scale (GDS) [38]; behavioral and psychological symptoms according to the neuropsychiatric inventory (NPI) [39], dementia diagnoses according to the ICD-10 diagnoses listed in the GP files, and the care level, assigned by the long-term care insurance for the amount of care and support a patient receives owing to their functional impairment, ranging from 1 to 5, with 1 indicating some problems and 5 indicating extreme problems.
2.2.2 Unmet Needs
As part of the DelpHi-Intervention, an algorithm-based intervention management system (IMS) was developed and embedded in the computer-assisted interview, tested, and evaluated following current dementia-specific guidelines to support the systematic identification of unmet needs [40]. The IMS is an expert decision support system operating on rule-based principles, aligning the unique attributes of PwD to a computerized knowledge base comprising validated questionnaires, tests, and tailored inquiries [11, 40]. An unmet need was either (1) recognized automatically by the IMS and checked for plausibility or (2) added manually by the dementia care manager following the principles of not having double-established services and not violating patients’ autonomy [11, 40].
Unmet needs were assigned to the following domains: (1) nursing treatment and care, (2) social counselling and legal support, (3) pharmaceutical treatment and care, (4) social integration and participation, (5) medical diagnosis and treatment, (6) special therapies, (7) others, and (8) caregiver support and education [11, 40]. The domain “others” contains specific needs that the DCM identified without matching the other predefined domains, such as participation in rehabilitation programs [11, 40]. The respective unmet needs were assessed dichotomously (present versus absent) and totaled for each domain, resulting in a count variable. An overview of the questionnaires used and the detailed technical structure of the IMS are published elsewhere [40].
2.2.3 Health-Related Quality of Life
HRQoL was assessed by using the EQ-5D‑5L [41, 42] as self- and, if available, as proxy ratings by participating family caregivers. The widely-used EQ-5D‑5L is a generic, preference-based, multidimensional instrument with five dimensions (mobility, self-care, pain/discomfort, usual activities, and anxiety/depression) and five levels (no, slight, moderate, severe, and extreme problems) accompanied by a thermometer-like visual analog scale (EQ-VAS) anchored by 0 (worst health) and 100 (best health) to assess health status at the time of assessment [41, 42]. The EQ-5D-5L responses were converted to health utility values using the German value set, anchored at 0 for death and 1 for full health [43]. Additionally, each of the mentioned dimensions was dichotomized (no versus any problem) to differentiate the problems experienced by patients in the physician network and DCC at baseline.
2.2.4 Health Resource Use and Costs
A prevalence-based bottom-up approach was used to first determine the extent of utilization of health resources and then to calculate the costs [44]. Health resource use was assessed retrospectively using the FIMA questionnaire [45] tailored to elderly individuals in the German healthcare system at baseline and 6 months after. Caregiver proxy ratings were captured to improve data validity, precision, and replacement in case of lacking plausibility or feasibility owing to advanced cognitive impairment. Detailed information about frequencies (number of visits, days stayed) or quantities of used medical (physician consultations, in-hospital care, drugs, aids, therapies) and formal care services (ambulatory care, day, and night care) were recorded. Healthcare costs were calculated from the payers perspective by using published standardized unit costs [inflated to 2022 and calculated in euros (€)] [46,47,48]. Informal care provided by patients’ informal caregivers was not included in this analysis. Supplementary Table 3 summarizes detailed information about the monetary valuation of the utilized services.
2.3 Statistical Analysis
Missing data was imputed using multiple imputations by chained equations (mice) separately for the respective healthcare setting. Only data from patients who received the intervention were imputed. Study participants sociodemographic and clinical characteristics, unmet needs, health resource use and costs, and HRQoL were presented using descriptive statistics. T tests (metric variables), Fisher exact tests (dichotomous variable), and Chi-square tests (categorical variable, > 2 conditions) were used to test for group differences between the settings (physician network versus DCC). In addition, dependent-sample t-tests were conducted for the unadjusted HRQoL and health resource utilization to examine changes within each setting over time.
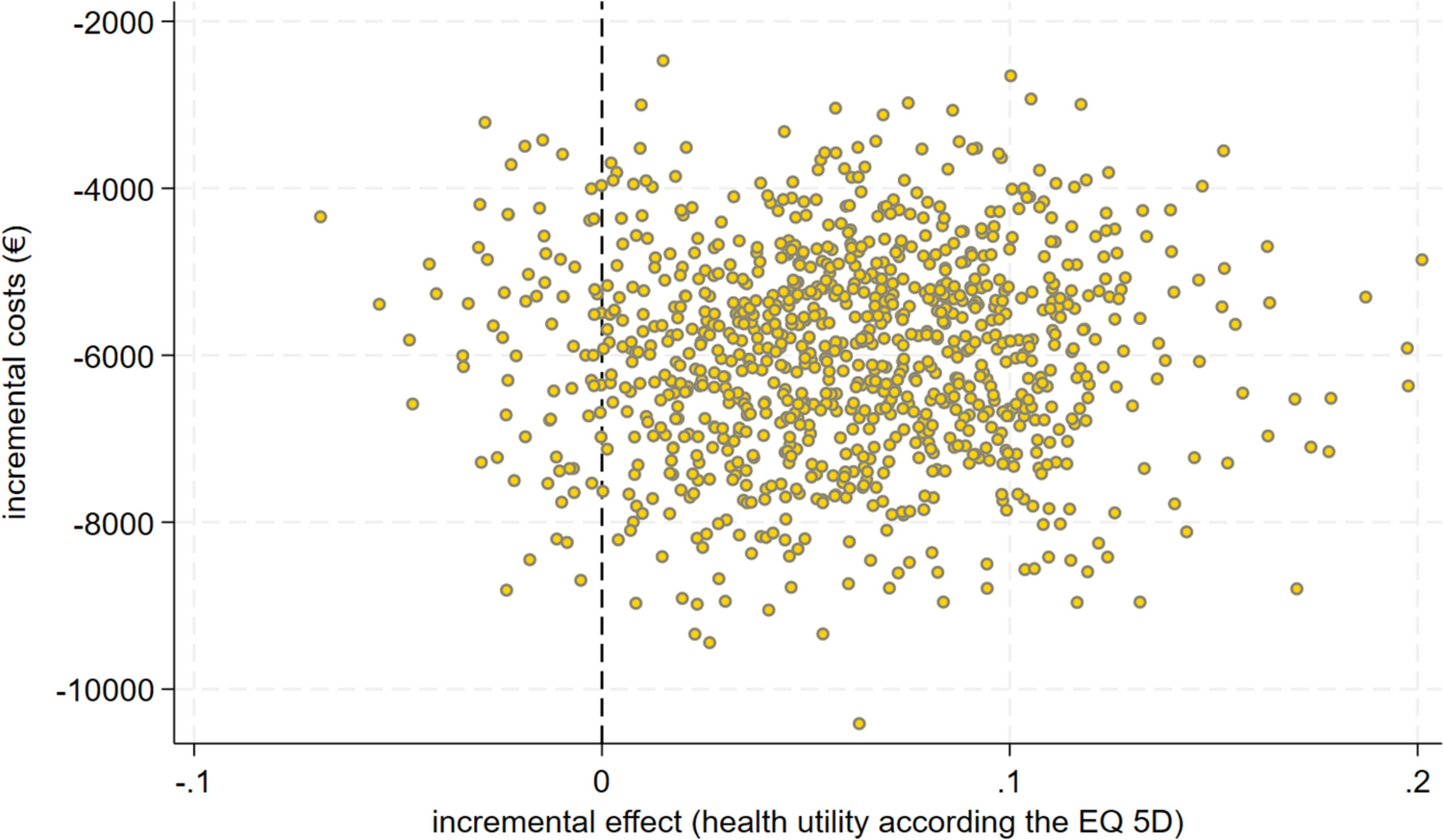
The incremental cost-effectiveness ratio (ICER) was calculated using the incremental cost per utility value on the basis of the EQ-5D-L gained to directly compare the respective settings cost-effectiveness. A total of N = 3 patients who had a health utility of zero died, and thus incurred no costs since the date of death. Healthcare costs and utility scores at follow-up were used as dependent variables, and the healthcare setting was used as a predictor of interest to predict the ICER. Multiple regression models were controlled for age, sex, living situation, and the respective value for healthcare costs (e.g., medication costs, therapy costs, or total costs) or utility scores at baseline. To handle sampling uncertainty in the ICER, nonparametric bootstrapping with 1000 resamples stratified for setting distribution was used to create the cost-effectiveness plane. For sensitivity analyses, quality-adjusted life-years (QALYs) based on the utility values for dyads [patients and participating caregivers (proxies)] were calculated, and cognitive impairment, according to the MMSE and functional impairment represented by the assigned care level through the long-term care insurance (dichotomous: no care level versus any care level) were considered.
Data analyses were on the basis of participants who completed the baseline and follow-up assessment or died after baseline. All statistical analyses were conducted with STATA/IC software, version 16 [49].






留言 (0)