Extragonadal germ cell tumors of the head and neck constitute about 5% of germ cell tumors [1,2,3]. Yolk sac tumors more frequently occur in gonadal sites than in extragonadal locations. Rare variants of malignant extragonadal germ cell tumors in the head and neck region include intracranial yolk sac tumors, primary orbital yolk sac tumors, and optic pathway yolk sac tumors [4]. Previous studies have reported that primary yolk sac tumors can involve different sites in the head and neck region including; the left pterygoid region, upper lip, para-pharyngeal and skull base, posterior fossa, floor of the mouth, and right masticator space and orbits [5,6,7,8,9,10,11].
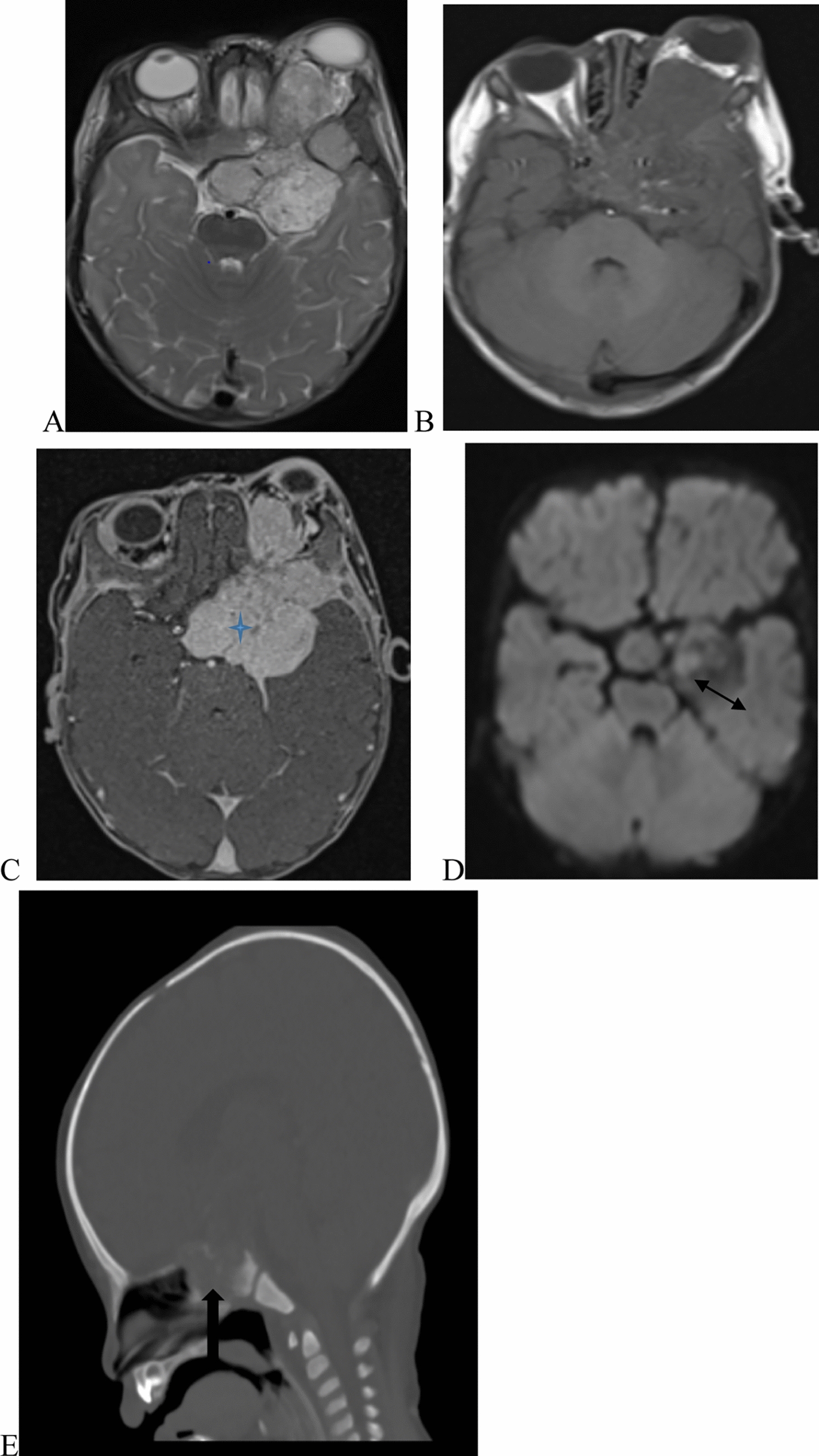
Radiographic features of this tumor were nonspecific with MRI findings of a heterogenous soft tissue mass in the orbit and surrounding tissues being reported. CT scans usually showed bony involvement with erosive changes with orbital involvement of variable degrees. [5, 7, 16,17,18]. The tissue biopsy and the CSF oncoproteins helped to reach the diagnosis in our case [12].
Thus, serum and CSF AFP are important tumor biomarkers for assessment of the therapeutic effect, and predictions of progressive disease or relapse during the follow-up period in children with yolk sac tumors. His pathologically, major histologic characteristics include Schiller-Duval bodies, a festoon-like pattern, a hepatoid pattern with hyaline globules, and a poly vesicular vitelline pattern, and immunohistochemically identified AFP is also a pivotal biomarker for the diagnosis of childhood yolk sac tumor [6, 11, 12].
The mainstay of treatment recommended for most extragonadal germ cell tumors in the intracranial and head and neck region includes a multidisciplinary approach including surgical resection of the mass and systemic chemotherapy [11]. A multiagent systemic chemotherapy regimen, including bleomycin, etoposide, cisplatin/carboplatin, cyclophosphamide, ifosfamide, vincristine, and 5-fluorouracil, has significantly improved the outcome of primary yolk sac tumors in the orbital region [12]. Radiation can be given as adjuvant and palliative management for advanced cases [1, 13,14,15].
In our case, the infant underwent radical left globe exenteration, left pterional craniotomy, and subtotal resection of the tumor. The histopathology and the AFP biomarkers confirmed the diagnosis of the primary intracranial yolk sac tumor. The child started on systemic multiagent chemotherapy with carboplatin, etoposide, and bleomycin, and took two cycles. But despite the multimodal therapy the child developed progressive disease and passed away after four months of diagnosis.





留言 (0)