This study was deemed exempt by the institutional review board at the University of Pennsylvania. No informed consent was required for this study. The study followed the Consolidated Health Economic Evaluation Reporting Standards (CHEERS).11
Data Source and Study Cohort
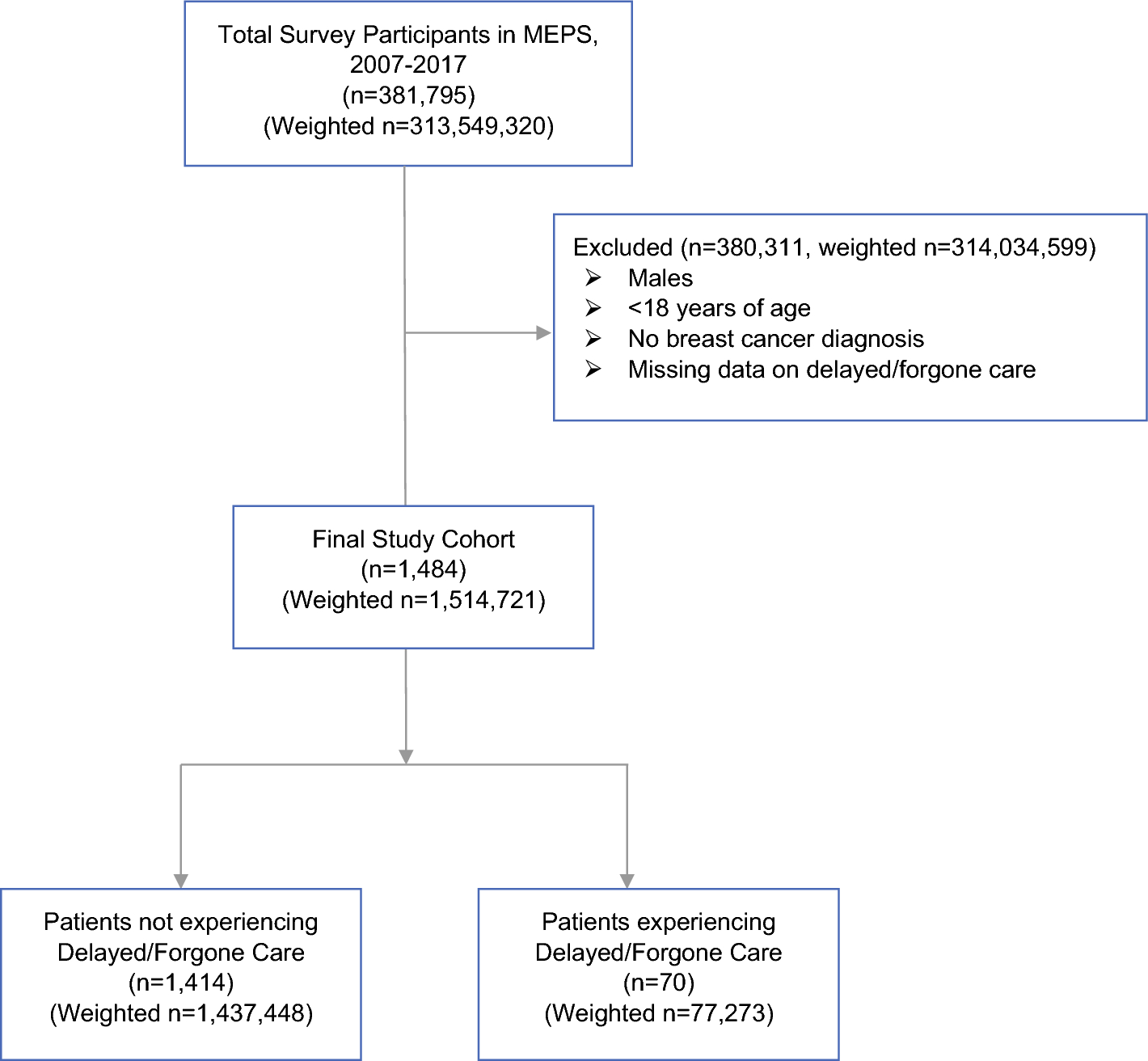
The Medical Expenditure Panel Survey (MEPS) is a series of nationally representative cross-sectional surveys that collect information from a sample of U.S. households on the sociodemographic and financial characteristics, medical conditions, health resource use, and associated costs of each household’s members. Respondents are each assigned a person-weight and variance estimation stratum to ensure national representativeness and adjust for unequal probabilities of selection, nonresponse, and other sampling biases. We collected annual full-year consolidated and medical conditions data files from MEPS for years 2007 to 2017. Full-year consolidated data files contain information on patients’ healthcare expenditures, healthcare encounters, sociodemographic characteristics, self-reported D/F necessary medical care, and self-reported reasons for D/F necessary medical care. Medical conditions files provide information on respondents’ medical conditions in the year preceding survey response in the form of International Classification of Diseases, 9th Edition, Clinical Modification (ICD-9-CM) and International Classification of Diseases, 10th Edition, Clinical Modification (ICD-10-CM) codes. Annual files were pooled together to obtain a large enough sample for determining precise estimates.
The study cohort included adult (age ≥ 18 years) females with a diagnosis of breast cancer in the 12 months preceding survey response, which was determined by ICD-9-CM codes 174 and 233 and ICD-10-CM code C50, and nonmissing data on D/F care.
Outcomes
The primary outcomes were self-reported D/F medical care, healthcare encounters, and healthcare expenditures in the 12-month period preceding the respondents’ completion of MEPS. Each participant was asked whether she had delayed necessary medical care in the preceding year (yes/no) and if she had forgone necessary medical care in the preceding year (yes/no). If a participant answered “yes” to either question, we considered her as having experienced D/F care. If a participant answered “yes” to either question, she was asked a follow-up question as to the reason for their D/F care. Reasons were classified as “financial,” “nonfinancial,” or “other” as detailed in Supplemental Methods 1.
To evaluate each participant’s healthcare encounters, we collected data on the number of emergency department (ED) visits, inpatient hospitalizations, outpatient visits, and office-based visits each participant had in the year preceding survey response. To evaluate each participant’s healthcare expenditures, we identified annual per capita total healthcare expenditures, out-of-pocket expenditures, ED expenditures, inpatient expenditures, outpatient expenditures, office-based visit expenditures, and prescription medication expenditures in the year preceding survey response. All expenditures were inflation-adjusted using values of the gross domestic product deflator obtained from the Organisation of Economic Co-operation and Development and are presented as constant 2017 U.S. dollars.
Statistical Analysis
Weighted baseline characteristics of the study cohort were summarized as counts (proportions) for categorical variables and medians (IQRs) for continuous variables. Baseline characteristics included age, race and ethnicity (Non-Hispanic [NH] White, NH Black, NH Asian, NH Other or Multiple Races, and Hispanic), family income as % of poverty line (poor or near poor [0–125%], low income [125–199%], middle income [200–399%], and high income [≥ 400%]), insurance type (private, public, and uninsured), educational attainment (less than GED, GED or high school diploma, and some college or more), census region of residence (northeast, midwest, south, west), and Charlson Comorbidity Index. Charlson Comorbidity Index was operationalized as a categorical variable (scores of 1, 2, and ≥ 3). Baseline characteristics among patients experiencing D/F care were compared with characteristics of those not experiencing D/F care using Rao-Scott adjusted chi-squared tests (for proportions) and Kruskal–Wallis tests (for medians).
To determine factors associated with experiencing D/F care, univariate unadjusted and multivariate adjusted logistic regression models were fit. Delayed/forgone care was the dependent variable. Age, race and ethnicity, family income as % of poverty line, insurance type, educational attainment, region, and Charlson Comorbidity Index were the independent variables. All logistic regression models accounted for survey weights and the complex survey design of MEPS.
To compare the frequency of healthcare encounters between those experiencing D/F care versus those who did not, unweighted proportions of patients having ≥ 1 ED visit, ≥ 1 hospitalization, and ≥ 1 outpatient visits were compared using Rao-Scott adjusted chi-squared tests. Because the distribution of office-based visits was not zero-inflated, proportions of respondents with 0–2, 2–5, and > 5 office-based visits were compared using Rao-Scott adjusted chi-squared tests. All proportions were compared first within the overall study cohort and subsequently within the following subgroups: respondents aged ≥ 65 years; respondents aged < 65 years; respondents whose family income was poor or near poor; and respondents whose family income was low, middle, or high.
Data on healthcare expenditures were zero-inflated. Therefore, two-part models were used to compare healthcare expenditures between those experiencing D/F care versus those who did not experience D/F care. The first part is a logit model that determines the probability of nonzero, positive expenditures. The second part is a generalized linear model with gamma distribution and logarithmic link function that estimates average annual per capita expenditures. Two-part models were separately fit to estimate each category of expenditures. The independent variable of interest was a binary variable indicating D/F care. All expenditure models were adjusted for insurance type, because insurance coverage was an independent, significant predictor of expenditures. The twopm command in Stata 18.0 was used to fit the two-part models, and average marginal effects were estimated by using the margins command. All expenditure models accounted for the complex survey design of MEPS. All models were constructed in Stata version 18.0 (Statacorp, USA). All statistical testing was 2-tailed, with P values < 0.05 considered statistically significant.



留言 (0)