
記住我
NHANES is a comprehensive examination program that evaluates the health and nutritional status of the U.S. population. This nationally representative survey uses a multistage, stratified sampling method to conduct thorough household interviews and physical examinations. It further collects additional information on demographics, lifestyles, dietary intake, behavioral situations, and medical status from US civilians every two years [14]. Detailed information regarding the survey sampling method and laboratory examinations can be found on the official website (http://www.cdc.gov/nchs/nhanes). The research protocol of NHANES was approved by the Ethics Review Board of the National Center for Health Statistics, and all participants provided written informed consent before participating in the study.
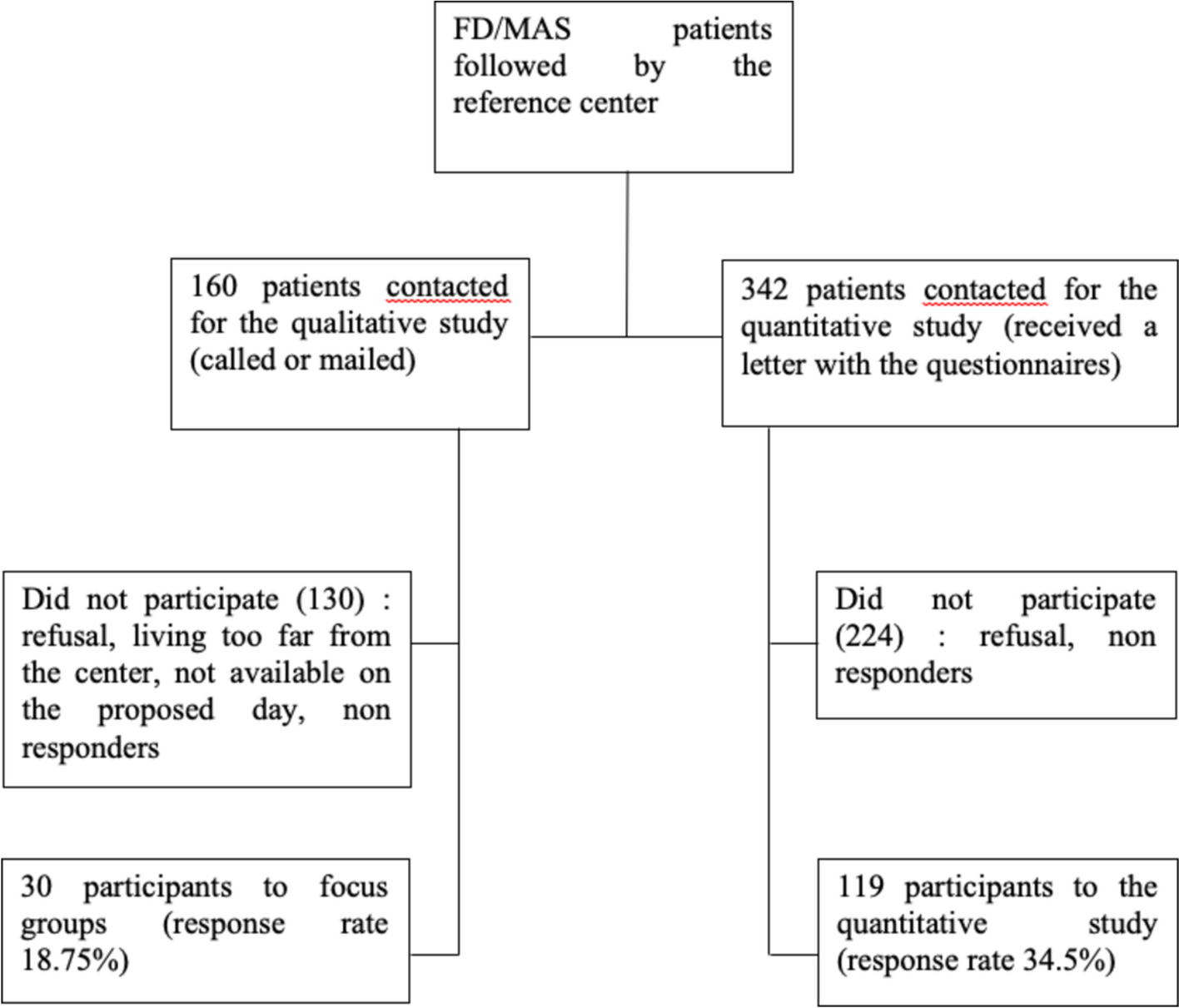
The present study was based on eight survey cycles of NHANES data from 2005 to 2020, encompassing a total of 76,496 individuals. Individuals who were younger than 50 years (n = 54,883), were corticosteroid users (n = 1085), did not undergo dual-energy X-ray absorptiometry (DXA) examination (n = 7467), or had missing data on dietary intake (n = 1058) were further excluded. Ultimately, 12,003 participants were included in the final analysis (Fig. 1).
Fig. 1
Flowchart of participant selection from NHANES 2005 to 2020
Outcome AssessmentDXA is the gold standard for assessing bone density, with detailed examination protocols available on the NHANES website. We collected the DXA scan results of the participants’ femoral neck or lumbar spine from NHANES 2005 to 2020. T scores were calculated via the following formula: T score = (BMD participant—mean BMD reference)/SD reference.
Here, BMD participant represents the participant’s measured BMD, the mean BMD reference represents the average BMD of the reference population, and the SD reference represents the standard deviation of peak BMD in the reference population. In the present study, the latest BMD data updated by Xue et al. [15] were adopted as a reference. Osteoporosis was defined as a T score ≤ −2.5, and osteopenia was defined as a T score between −2.5 and −1 at the femoral neck or lumbar spine. LBMD includes both osteoporosis and osteopenia and is defined as a T score ≤ −1 at the femoral neck or lumbar spine.
Assessment of Dietary Tryptophan IntakeThe dietary interview component of NHANES reports two 24-h dietary recall interviews for each participant. The first dietary recall is conducted in person at the Mobile Examination Center, whereas the second 24-h recall is collected via telephone interview 3–10 days later. The USDA Food and Nutrient Database for Dietary Studies was used to calculate the nutrient and food components of all foods. The mean of the participants’ two dietary recalls, or the value of one of them (if participants had only one recall), was used as the daily dietary tryptophan intake to mitigate potential recall bias in this study. Dietary tryptophan intake was natural log transformed to minimize the effect of outliers and improve the interpretability of the association results.
Covariates AssessmentIndividual characteristics, such as sex (male and female), age (< 65 years and ≥ 65 years), race/ethnicity (Mexican American, Non-Hispanic White, Non-Hispanic Black, and Other), educational level (below high school, high school or equivalent, and college education or above), marital status (single, widowed or divorced, and married), the family poverty income ratio (PIR ≤ 1.3, 1.3–3.5, and ≥ 3.5), physical activity level (inactive, moderate, and active), alcohol consumption (ever consumed 12 drinks), smoking history (ever smoked 100 cigarettes), and milk intake (never or rarely, sometimes, and often), were self-reported. The weight and height of each participant were obtained through physical examination, and body mass index (BMI) was calculated as weight (kg)/height (m2). Medical history, including diabetes, hypertension, hyperlipidemia, stroke, and cardiovascular disease (CVD), was evaluated through self-reports, medication use, or dietary changes due to these conditions. Blood biochemical indicators such as alanine aminotransaminase (ALT), aspartate aminotransaminase (AST), fasting plasma glucose (FPG), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), serum phosphorus, and calcium were also included, with detection methods available on the official website. Additionally, other dietary intake values, including energy, protein, carbohydrates, total fat, sugar, fiber, cholesterol, vitamin B6, vitamin B12, choline, folate, calcium, and phosphorus were considered continuous covariates in the analysis.
Statistical AnalysisThe complex weighting of NHANES data was performed using the “survey” package in R, with “WTDRD1” or “WTDR2D” used to calculate sample weights from 2005 to 2020. The participants were grouped on the basis of the presence of LBMD and quartiles of dietary tryptophan intake (natural log transformed). Continuous variables, if normally distributed, are represented as the mean ± standard deviation (SD) and were compared using the Student’s t test (for two groups); otherwise, the median with interquartile range (IQR) and the Wilcoxon rank-sum test were employed. Categorical variables are presented as numbers (weighted proportions) and were analyzed using the chi-square test.
Weighted multivariable logistic regression models were used to investigate the link between dietary tryptophan intake (as a continuous variable or in quartiles) and the risk of LBMD, and odds ratios (OR) along with 95% confidence interval (CI) were reported. Four models were created: Model 1 did not make any adjustments; Model 2 adjusted for age, sex, and race/ethnicity; Model 3 adjusted for age, sex, race and ethnicity, BMI, educational level, marital status, PIR, alcohol consumption, diabetes, FPG, TC, LDL-C, HDL-C, ALT, AST, and serum phosphorus; and Model 4 adjusted for the variables in Model 3 plus nutritional elements, including energy, protein, carbohydrate, sugars, fiber, fat, cholesterol, vitamin B6, vitamin B12, folate, choline, calcium, and phosphorus. Restricted cubic splines (RCS) were applied to explore the potentially nonlinear relationship between dietary tryptophan intake and LBMD, with adjustments in Model 4.
In the primary analysis, multiple imputation was used to address missing covariates. To ensure the robustness of our study, sensitivity analyses were conducted. These included analyzing the remaining four imputed datasets, excluding individuals with missing covariates, excluding participants with only one dietary recall, and adjusting tryptophan intake using the nutrient residual method after controlling for energy intake. All analyses were performed using R software (version 4.3.2; https://www.R-project.org) and a two-tailed p value < 0.05 was considered statistically significant.
留言 (0)