
記住我







In 2021, there were 173.9 million malaria cases (95% UI: 158.0, 194.5) worldwide, representing an increase of 9.0% compared with 1990, and the global age-standardized prevalence rate for malaria was 2336.8 per 100,000 population (95% UI: 2122.9, 2612.2 per 100,000 population), with a decrease of − 16.5% (95% UI: − 26.4, − 5.3%) compared with 1990, and there was no upwards or downwards trend (P > 0.05). The global age-standardized DALYs rate for malaria was estimated at 806.0 per 100,000 population (95% UI: 318.9, 1570.2 per 100,000 population), with a percentage change of −16.5% (95% UI: − 36.8, 2.5%), compared with 1990, and there was no significant upwards or downwards trend (P > 0.05) (Table 1). In the past 30 years, the age-standardized prevalence rate of malaria has declined in high-SDI regions (% change = − 77.1, 95% UI: − 86.5, − 61.0), high-middle-SDI regions (% change = − 81.2, 95% UI: − 90.6, − 65.6), middle-SDI regions (% change = − 36.4, 95% UI: − 57.0, − 5.0), low-middle-SDI regions (% change = − 41.7, 95% UI: − 52.8, − 29.5), and low-SDI regions (% change = − 44.9, 95% UI: − 53.4, − 35.6), and there has been a significant downwards trend across various SDI categories (P < 0.05). Malaria was most prevalent across the GBD central sub-Saharan Africa, at 21,328.8 per 100,000 population (95% UI: 16,092.3, 28,557.4 per 100,000 population), and 38,056.5 per 100,000 population (95% UI: 33,491.8, 42,691.8 per 100,000 population) in 1990. Andean Latin America, central Asia, East Asia, and southern Latin America had the largest declines (more than 80%) in malaria prevalence over the past 30 years. The age-standardized DALYs rate significantly declined in the high-SDI regions (% change = − 94.2, 95% UI: − 96.5, − 89.7), which showed a pronounced downwards trend (P < 0.05). However, the age-standardized DALYs rate for malaria remained relatively high in western sub-Saharan Africa, central sub-Saharan Africa, and eastern sub-Saharan Africa (Table 1).
Table 1 Age-standardized prevalence rate and DALYs rate for malaria in 1990 and 2021 and the percentage change in the age-standardized rates per 100,000 population by GBD region from 1990–2021In 2021, there were 6.2 million cases of leishmaniasis worldwide (95% UI: 5.8, 6.7), representing an increase of 95.0% from 1990, and the global age-standardized prevalence rate was 77.0 per 100,000 population (95% UI: 71.9, 83.0 per 100,000 population), up by 22.3% (95% UI: 5.8, 40.5%) from 1990, with no significant upwards or downwards trend (P > 0.05). The global age-standardized DALYs rate was 10.3 per 100,000 population (95% UI: 6.0, 22.0 per 100,000 population), with a percentage change of −87.1% (95% UI: −91.7, −76.7%), compared with 1990, with a significant downwards trend (P < 0.05) (Table 2). Over the past 30 years, the age-standardized prevalence rate has declined in high-middle-SDI regions (% change = − 0.4%, 95% UI: − 30.6, 53.8) and low-middle-SDI regions (% change = − 26.8, 95% UI: − 39.9, − 12.4), and there has been no upwards or downwards trend, P > 0.05. However, it increased in the high-SDI regions (% change = 18.1, 95% UI: − 21.2, 129.3), middle-SDI regions (% change = 26.6, 95% UI: − 1.0, 59.4), and low-SDI regions (% change = 42.0, 95% UI: 1.6, 97.5). Leishmaniasis was most prevalent across GBD North Africa and the Middle East region, with a rate of 642.9 per 100,000 population (95% UI: 592.1, 712.9 per 100,000 population) in 2021, and it slightly decreased from 645.7 per 100,000 population (95% UI: 480.8, 883.7 per 100,000 population) in 1990. The age-standardized DALYs rate decreased in the high-SDI regions (% change = − 23.5, 95% UI: − 75.2, 99.0), high-middle-SDI regions (% change = − 74.6, 95% UI: − 90.7, 25.0), middle-SDI regions (% change = − 40.5, 95% UI: − 75.4, 47.7), low-middle-SDI regions (% change = − 83.3, 95% UI: − 89.3, − 61.0), and low-SDI regions (% change = − 95.0, 95% UI: − 96.8, − 91.3), and there was a significant downwards trend in the low-SDI regions (P < 0.05). However, the age-standardized DALYs rate for leishmaniasis was higher in tropical Latin America, North Africa, the Middle East, and Andean Latin America than in other regions (Table 2).
Table 2 Age-standardized prevalence rate and DALYs rate for leishmaniasis in 1990 and 2021 and the percentage change in the age-standardized rates per 100,000 population by GBD region from 1990–2021For lymphatic filariasis, there were 56.9 million cases (95% UI: 48.7, 67.9) globally, representing a decrease of 72.8% compared with 1990, and the estimated global age-standardized prevalence rate was estimated at 706.0 per 100,000 population (95% UI: 603.7, 841.8 per 100,000 population) in 2021, with a decrease of − 82.6% (95% UI: − 85.8, − 78.7%) compared with 1990. In 2021, the global age-standardized DALYs rate was estimated at 16.5 per 100,000 population (95% UI: 9.7, 28.0 per 100,000 population), which was a decrease of − 79.1% (95% UI: − 84.2, − 70.5%) compared with that in 1990 (Table 3). Lymphatic filariasis was most prevalent across GBD Oceania, with 7646.7 per 100,000 population (95% UI: 2970.4, 18,140.4 per 100,000 population) in 2021 and a decrease from 33,028.4 per 100,000 population (95% UI: 17,334.7, 52,695.9 per 100,000 population) in 1990. Oceania and southern sub-Saharan Africa also experienced declines in the prevalence of malaria. Additionally, over the past 30 years, the age-standardized prevalence rate of lymphatic filariasis decreased in the high-middle-SDI regions (% change = − 70.7, 95% UI: − 90.0, − 15.2), middle-SDI regions (% change = − 82.7, 95% UI: − 89.4, − 72.3), low-middle-SDI regions (% change = − 85.9, 95% UI: − 88.6, − 82.6), and low-SDI regions (% change = − 88.4, 95% UI: − 90.9, − 85.7), and the age-standardized DALYs rate also decreased in the high-middle-SDI regions (% change = − 59.3, 95% UI: − 68.8, − 44.2), middle-SDI regions (% change = − 79.5, 95% UI: − 84.6, − 70.7), low-middle-SDI regions (% change = − 83.9, 95% UI: − 87.8, − 77.8), and low-SDI regions (% change = − 86.6, 95% UI: − 90.1, − 80.8). However, the age-standardized DALYs rate for lymphatic filariasis was higher in Oceania, western sub-Saharan Africa, South Asia, and central sub-Saharan Africa (Table 3).
Table 3 Age-standardized prevalence rate and DALYs rate for lymphatic filariasis in 1990 and 2021 and the percentage change in the age-standardized rates per 100,000 population by GBD region from 1990–2021For African trypanosomiasis, there were 2367.9 cases (95% UI: 1130.4, 4391.7) globally, representing a decrease of 96.2% compared with 1990, and the global age-standardized prevalence rate was estimated at 0.03 per 100,000 population (95% UI: 0.01, 0.06 per 100,000 population) in 2021, decreasing by − 97.4% (95% UI: − 97.7, − 97.2%) compared with 1990, and there was a significant downwards trend (P < 0.05). The global age-standardized DALYs rate was 0.8 per 100,000 population (95% UI: 0.3, 2.3 per 100,000 population), with a percentage change of − 96.0% (95% UI: − 97.8, − 89.8%) compared with that in 1990, and there was a significant downwards trend (P < 0.05) (Table 4). From 1990–2021, the age-standardized prevalence rate of African trypanosomiasis declined in middle-SDI regions (% change = − 80.6, 95% UI: − 83.0, − 77.3), low-middle-SDI regions (% change = − 97.3, 95% UI: − 97.6, − 96.9), and low-SDI regions (% change = − 98.7, 95% UI: − 98.9, − 98.5), and there was a significant downwards trend in these regions (P < 0.05). The age-standardized DALYs rate also declined in the middle-SDI regions (% change = − 84.1, 95% UI: − 90.7, − 73.9), low-middle-SDI regions (% change = − 96.2, 95% UI: − 97.7, − 92.2), and low-SDI regions (% change = − 97.9, 95% UI: − 99.0, − 93.6), and there was a significant downwards trend in these regions, (P < 0.05). Notably, owing to the low prevalence of African trypanosomiasis in high-SDI regions, high-middle-SDI regions and some countries or insufficient research focus, there was a lack of relevant data in the GBD database used, which prevented accurate estimation (Table 4).
Table 4 Age-standardized prevalence rates and DALY rates for African trypanosomiasis in 1990 and 2021 and the percentage change in the age-standardized rates per 100,000 population by GBD region from 1990–2021In 2021, 6.3 million people (95% UI: 5.4, 7.2) worldwide had Chagas disease, representing a decrease of 10.9% compared with 1990, and the estimated global age-standardized prevalence rate of Chagas disease in 2021 was 75.6 per 100,000 population (95% UI: 65.2, 86.5 per 100,000 population), with a percentage change of − 47.9% (95% UI: − 49.3, − 46.4%) compared with 1990, and there was a pronounced downwards trend (P < 0.05). Chagas disease was most prevalent across the GBD Southern Latin America, at 1346.1 per 100,000 population (95% UI: 1176.1, 1538.4 per 100,000 population) in 2021, with a decrease from 3944.8 per 100,000 population (95% UI: 3466.5, 4402.7 per 100,000 population) in 1990, followed by Andean Latin America, tropical Latin America, and Central Latin America, with a certain distribution pattern (Table 5). In 2021, the estimated global age-standardized DALYs rate was 2.8 per 100,000 population (95% UI: 2.4, 3.2 per 100,000 population), with a decline of −71.2% (95% UI: − 74.7, − 67.0%) compared with 1990, and there was a significant decrease (P < 0.05). Over the past 30 years, the age-standardized incidence rate of Chagas disease has declined in high-middle-SDI regions (% change = − 60.3, 95% UI: − 62.5, − 58.1), middle-SDI regions (% change = − 46.6, 95% UI: − 48.7, − 44.1), and low-middle-SDI regions (% change = − 48.1, 95% UI: − 50.4, − 46.0), and there has been a pronounced downwards trend in those regions (P < 0.05). Andean Latin America, Australasia, the Caribbean, central Latin America, southern Latin America, and tropical Latin America experienced decreases in the prevalence of Chagas disease. The age-standardized DALYs rate decreased in the high-SDI regions (% change = − 17.7, 95% UI: − 25.1, − 11.0), high-middle-SDI regions (% change = − 72.8, 95% UI: − 77.8, − 66.0), middle-SDI regions (% change = − 77.8, 95% UI: − 80.6, − 74.2), and low-middle-SDI regions (% change = − 64.7, 95% UI: − 71.1, − 56.1), and there were pronounced downwards trends in the high-middle-SDI regions, middle-SDI regions, and low-middle-SDI regions (P < 0.05) (Table 5).
Table 5 Age-standardized prevalence rates and DALY rates for Chagas disease in 1990 and 2021 and the percentage change in the age-standardized rates per 100,000 population by GBD region from 1990–2020For onchocerciasis, there were 19.6 million cases (95% UI: 17.8, 21.7) globally, representing a decrease of 16.3% compared with 1990, and the age-standardized prevalence rate was estimated at 246.2 per 100,000 population (95% UI: 222.7, 273.1 per 100,000 population) in 2021, decreasing by − 44.6% (95% UI: − 46.6, − 42.6%) compared with 1990. Notably, the disease burden was still high in specific areas, such as central sub-Saharan Africa, eastern sub-Saharan Africa and western sub-Saharan Africa, reflecting a certain distribution pattern (Table 6). Onchocerciasis was most prevalent across the GBD central sub-Saharan Africa, with 9857.7 per 100,000 population (95% UI: 9222.2, 10,576.1 per 100,000 population) in 2021 and a decrease from 18,426.1 per 100,000 population (95% UI: 17,260.6, 19,762.9 per 100,000 population) in 1990. Over the past 30 years, the age-standardized prevalence rate decreased in the middle-SDI regions (% change = − 68.1, 95% UI: − 74.3, − 61.5), low-middle-SDI regions (% change = − 73.2, 95% UI: − 76.4, − 70.1), and low-SDI regions (% change = − 59.3, 95% UI: − 59.9, − 58.7). The age-standardized prevalence rate of low-SDI regions was 1728.6 per 100,000 population (95% UI: 1593.1, 1892.1 per 100,000 population) in 2021, which was still the highest across all SDI levels. The estimated global age-standardized DALYs rate of onchocerciasis was 15.8 per 100,000 population (95% UI: 9.4, 23.9 per 100,000 population), with a percentage change of − 40.8% (95% UI: − 45.0, − 37.1%) compared with that in 1990, but there was no upwards or downwards trend (P > 0.05). From 1990–2021, the estimated global age-standardized DALYs rate of onchocerciasis declined in the middle-SDI regions (% change = − 61.7, 95% UI: − 72.0, − 50.4), low-middle-SDI regions (% change = − 66.3, 95% UI: − 71.9, − 60.6), and low-SDI regions (% change = − 56.9, 95% UI: − 58.2, − 55.4), and there was a pronounced downwards trend in the low-middle-SDI regions, (P < 0.05) (Table 6).
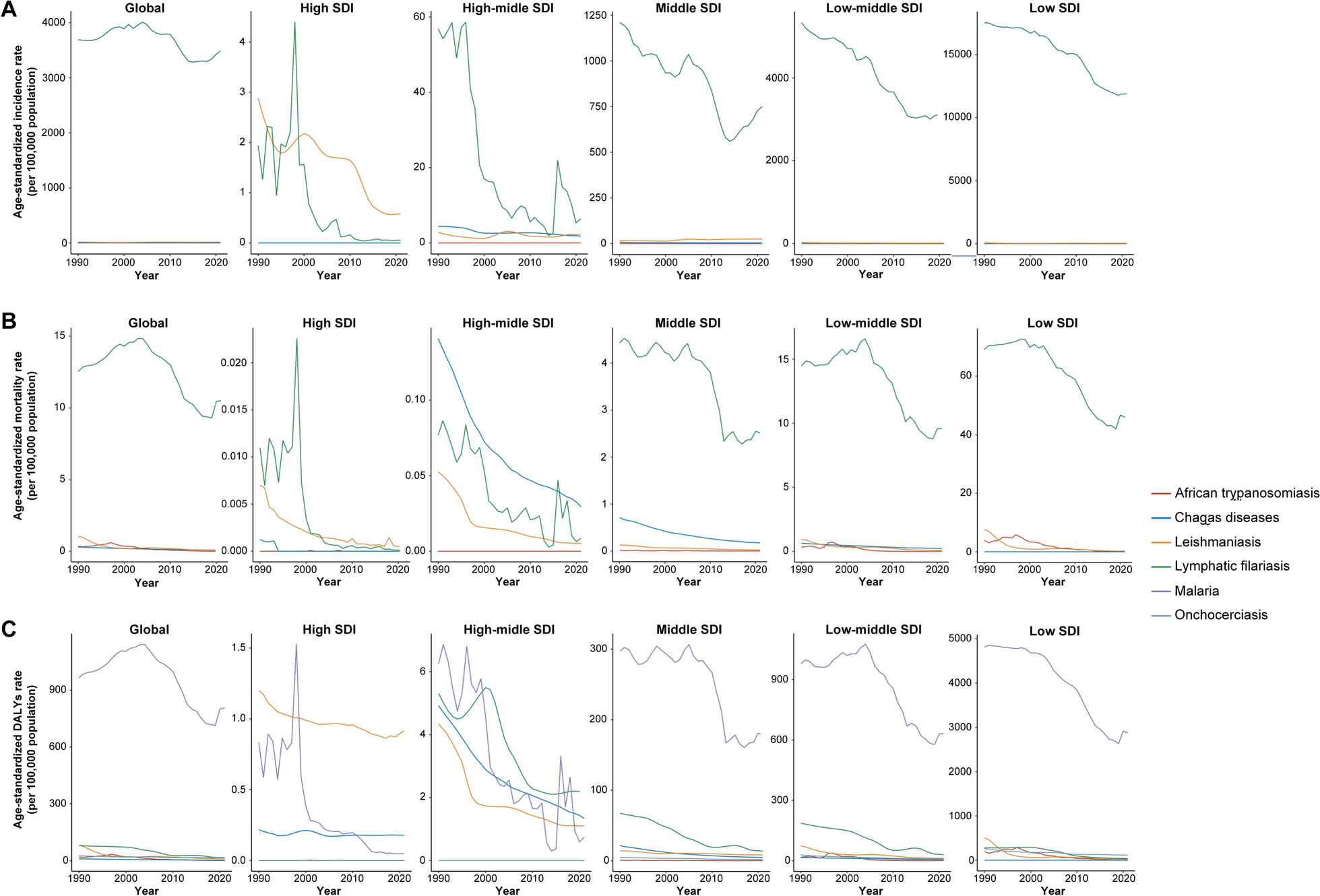
Table 6 Age-standardized prevalence rates and DALY rates for onchocerciasis in 1990 and 2021 and the percentage change in the age-standardized rates per 100,000 population by GBD region from 1990–2021Association between the burden of the vb-pIDP and the SDIOverall, over the past 30 years, the age-standardized prevalence rate and DALYs rate for malaria, leishmaniasis, lymphatic filariasis, African trypanosomiasis, Chagas disease, and onchocerciasis have shown declining trends globally and in regions with different SDI levels (Fig. 1).
Fig. 1
Age-standardized prevalence rate and DALYs rate of vb-pIDP globally and across all SDI quintiles, 1990–2021. A Malaria. B Leishmaniasis. C Lymphatic filariasis. D African trypanosomiasis. E Chagas disease. F Onchocerciasis. SDI sociodemographic index, Vb-IDP vector-borne infectious disease of poverty
For malaria, the age-standardized prevalence rate and DALYs rate have decreased globally and across all SDI levels, with the most significant decline occurring in low-SDI regions. In the low-SDI regions, the age-standardized prevalence decreased from 17,155.4 per 100,000 population (95% UI: 15,844.1, 18,797.5 per 100,000 population) in 1990 to 9458.6 per 100,000 population (95% UI: 8494.2, 10,473.8 per 100,000 population) in 2021, whereas the age-standardized DALYs rate decreased from 4811.5 per 100,000 population (95% UI: 2580.7, 8569.1 per 100,000 population) in 1990 to 2869.2 per 100,000 population (95% UI: 1107.4, 5683.9 per 100,000 population) in 2021 and was still significantly higher than that in other SDI level regions (Fig. 1A, Table 1). Over the past 30 years, the age-standardized prevalence rates were higher than expected on the basis of the SDI at the global level and in central sub-Saharan Africa, Oceania, western sub-Saharan Africa, and eastern sub-Saharan Africa. Additionally, the age-standardized DALYs rates were higher than expected on the basis of the SDI at the global level and in central sub-Saharan Africa, western sub-Saharan Africa, and southern sub-Saharan Africa during the same period (Fig. 2A).
Fig. 2
Age-standardized prevalence rate and DALYs rate of vb-pIDP, globally and for 21 GBD regions, by SDI, 1990–2021. A Malaria. B Leishmaniasis. C Lymphatic filariasis. D African trypanosomiasis. E Chagas disease. F Onchocerciasis. Every dot represents a specific year between 1900 and 2021, and its color implies the geographic region. SDI sociodemographic index, Vb-IDP vector-borne infectious disease of poverty
For leishmaniasis, the overall age-standardized prevalence rate fluctuated from 1990–2021. The age-standardized prevalence rate decreased only in the high-SDI regions, whereas it increased globally and, in the middle-SDI and low-SDI regions (Fig. 1B). Overall, the age-standardized DALYs rate for leishmaniasis decreased globally from 1990–2021. In particular, there was a higher age-standardized DALYs rate in the low-SDI regions than in the other regions in 1990, but it significantly declined over time and stabilized by 2021. The age-standardized DALYs rate of low-SDI regions decreased by − 95.0% (95% UI: − 96.8, − 91.3) (Table 2). In other regions, the age-standardized DALYs rates were relatively low and gradually decreased. Over the past 30 years, the age-standardized prevalence rates were higher than expected on the basis of the SDI in North Africa and the Middle East, Andean Latin America, tropical Latin America, central Latin America, and central Asia. Additionally, the age-standardized DALYs rates were higher than expected on the basis of the SDI in tropical Latin America, North Africa, the Middle East, and Andean Latin America (Fig. 2B).
From 1990–2021, the age-standardized prevalence rate and DALYs rate for lymphatic filariasis declined globally, as did the rates in the low-SDI, low-middle-SDI, and middle-SDI regions, with some fluctuations (Fig. 1C). The age-standardized prevalence rate and DALYs rate of lymphatic filariasis decreased most significantly in the low-SDI regions, followed by the low-middle-SDI regions. The age-standardized prevalence rate decreased by − 88.4% (95% UI: − 90.9, − 85.7) and the age-standardized DALYs rate decreased by − 86.6% (95% UI: − 90.1, − 80.8) in low-SDI regions (Table 3). However, the age-standardized prevalence rate and DALYs rate remained extremely low and stable in high-SDI and high-middle-SDI regions. Additionally, the age-standardized prevalence rate and DALYs rate were higher than expected on the basis of the SDI at the global level and in Oceania, southeast Asia, the Caribbean, South Asia, and western sub-Saharan Africa (Fig. 2C).
For African trypanosomiasis, the age-standardized prevalence rate and DALYs rate rapidly increased after 1990, peaked in approximately 1996, then significantly declined and stabilized by 2021 in low-SDI regions. In contrast, the age-standardized prevalence rate and DALYs rate were relatively low in other regions, with overall gradual but declining trends (Fig. 1D). From 1990–2021, the age-standardized prevalence rate and DALYs rate in central sub-Saharan Africa were significantly higher than expected (Fig. 2D). The age-standardized prevalence rate of African trypanosomiasis was 94.4 per 100,000 population (95% UI: 41.7, 183.2) compared with the global average of 1.2 per 100,000 population (95% UI: 0.5, 2.2) in 1990, and the age-standardized prevalence rate was 0.9 per 100,000 population (95% UI: 0.5, 1.6) compared with the global average of 0.03 per 100,000 population (95% UI: 0.01, 0.06) in 2021. The age-standardized DALYs rate of African trypanosomiasis was 1181.1 per 100,000 population (95% UI: 585.3, 1964.8) compared with the global average of 19.9 per 100,000 population (95% UI: 10.0, 31.9), and the age-standardized DALYs rate was 15.0 per 100,000 population (95% UI: 7.4, 25.9) compared with the global average of 0.8 per 100,000 population (95% UI: 0.3, 2.3) (Table 4).
Over the past 30 years, both the age-standardized prevalence rate and DALYs rate of Chagas disease have declined globally, as have those of high–middle-SDI, middle-SDI, and low–middle-SDI regions, and stabilized by 2021 (Fig. 1E). From 1990–2021, the age-standardized prevalence rate and DALYs rate in southern Latin America, tropical Latin America, Andean Latin America, and central Latin America were significantly higher than expected (Fig. 2E). For example, the age-standardized prevalence of Central Latin America was 1516.2 per 100,000 population (95% UI: 1277.2, 1810.2) compared with the global average of 145.2 per 100,000 population (95% UI: 125.4, 168.3) in 1990, and the age-standardized prevalence rate was 791.0 per 100,000 population (95% UI: 663.3, 920.2) compared with 75.6 per 100,000 population (95% UI: 65.2, 86.5) in 2021. The age-standardized DALYs rate of Central Latin America was 14.2 per 100,000 population (95% UI: 9.9, 19.6) compared with the global average of 26.7 per 100,000 population (95% UI: 16.0, 40.0) in 1990, and the age-standardized DALYs rate was 0.2 per 100,000 population (95% UI: 0.1, 0.3) compared with the global average of 15.8 per 100,000 population (95% UI: 9.4, 23.9) in 2021 (Table 5). The global age-standardized prevalence and DALYs rate for onchocerciasis have declined and fluctuated, with the most significant decrease observed. The age-standardized prevalence rate of onchocerciasis decreased by − 0.6% (95% UI: − 0.6, − 0.6) and the age-standardized DALYs rate decreased by − 0.57% (95% UI: − 0.58, − 0.55) (Fig. 1F, Table 6). Additionally, the age-standardized prevalence rates were higher than expected on the basis of the SDI in southeast Asia and central sub-Saharan Africa, and the age-standardized DALYs rate in central sub-Saharan Africa was higher than expected (Fig. 2F).
In 2021, there were negative correlations between the age-standardized prevalence rates of malaria (R = − 0.7230, P = 3.270e−67), leishmaniasis (R = − 0.2632, P = 6.852e−08), African trypanosomiasis (R = − 0.3141, P = 8.533e−11), lymphatic filariasis (R = − 0.5894, P = 1.572e−39), and onchocerciasis (R = − 0.5179, R = 2.223e−29) and the SDI, with the prevalence decreasing significantly as the SDI increased (Fig. 3A–D, F). There were negative correlations between the age-standardized DALYs rates for malaria (R = − 0.7688, P = 4.372e−41), leishmaniasis (R = − 0.3329, P = 1.140e−06), African trypanosomiasis (R = − 0.3134, P = 5.002e−06), lymphatic filariasis (R = − 0.5716, P = 4.335e−19), and onchocerciasis (R = − 0.5192, P = 1.764e−15) and the SDI, with the burden decreasing significantly as the SDI increased (Fig. 3A–D, F). However, for Chagas disease, there were positive correlations between the age-standardized prevalence (R = 0.3195, P = 3.893e−11) and DALYs (R = 0.2989, P = 14.05e−05) rates and the SDI (Fig. 3E).
Fig. 3
Age-standardized prevalence rate and DALYs rate of vb-pIDP in 204 countries with different SDI levels in 2021. A Malaria. B Leishmaniasis. C Lymphatic filariasis. D African trypanosomiasis. E Chagas disease. F Onchocerciasis. Every dot represents the prevalence rate of a country, and its color has been chosen arbitrarily without any implications for the geographic region. CAR Central African Republic, DRC Democratic Republic of the Congo, SDI sociodemographic index, Vb-pIDP vector-borne infectious disease of poverty
Gender and age distribution for the vb-pIDPThe specific prevalence rates for malaria, leishmaniasis, African trypanosomiasis, Chagas disease, and onchocerciasis and the specific DALYs rates for malaria, leishmaniasis, African trypanosomiasis, and onchocerciasis were not different between males and females across all age groups (P > 0.05) (Fig. 4A, B, D–F). For lymphatic filariasis, in the 15–19 years age group and above, the specific DALYs rates were higher in females than in males (P < 0.05), with no differences in the other age groups (P > 0.05) (Fig. 4C). Conversely, in the 35–39, 40–44, 45–49, 50–54, 55–59, and 60–64 age groups, the specific DALYs rates for Chagas disease were higher in males than in females (P < 0.05), with no differences in the other age groups (P > 0.05) (Fig. 4C).
Fig. 4
Age-standardized prevalence and DALYs rate of vb-pIDP in different age groups in 2021. A Malaria. B Leishmaniasis. C Lymphatic filariasis. D African trypanosomiasis. E Chagas disease. F Onchocerciasis. SDI sociodemographic index, Vb-pIDP vector-borne infectious diseases of poverty, DALYs disability-adjusted life years.
The specific prevalence rate and DALYs rate of malaria were highest in children under five years of age and decreased with increasing age (Fig. 4A). The number of cases and DALYs rate of lymphatic filariasis peaked in the 20–24 years age group and then gradually declined with increasing age, and the number of malaria cases and DALYs rate peaked in the 15–19 years age group and then gradually declined with increasing age (Fig. 4C). For African trypanosomiasis, overall, the DALYs rate was relatively low in children under the age of five years, started to gradually increase from the age of 5 years, peaked at 20–24 years, then gradually decreased, and then continued to decline with increasing age (Fig. 4D).
Variance analysis in 21 geographic regions of the globeIn 2021, among the six vb-pIDP, malaria had the highest age-standardized prevalence rate and DALYs rate globally, followed by lymphatic filariasis. Furthermore, malaria had the highest age-standardized prevalence and DALYs rate in western sub-Saharan Africa and central sub-Saharan Africa, followed by eastern sub-Saharan Africa and Oceania (Additional file 1: Figure S1). Notably, lymphatic filariasis had the highest age-standardized prevalence rate in Oceania, whereas onchocerciasis had the highest age-standardized prevalence rate in central sub-Saharan Africa (Additional file 1: Figure S1A). The age-standardized DALYs rate of onchocerciasis was higher in central sub-Saharan Africa than in other regions of the world (Additional file 1: Figure S1B).
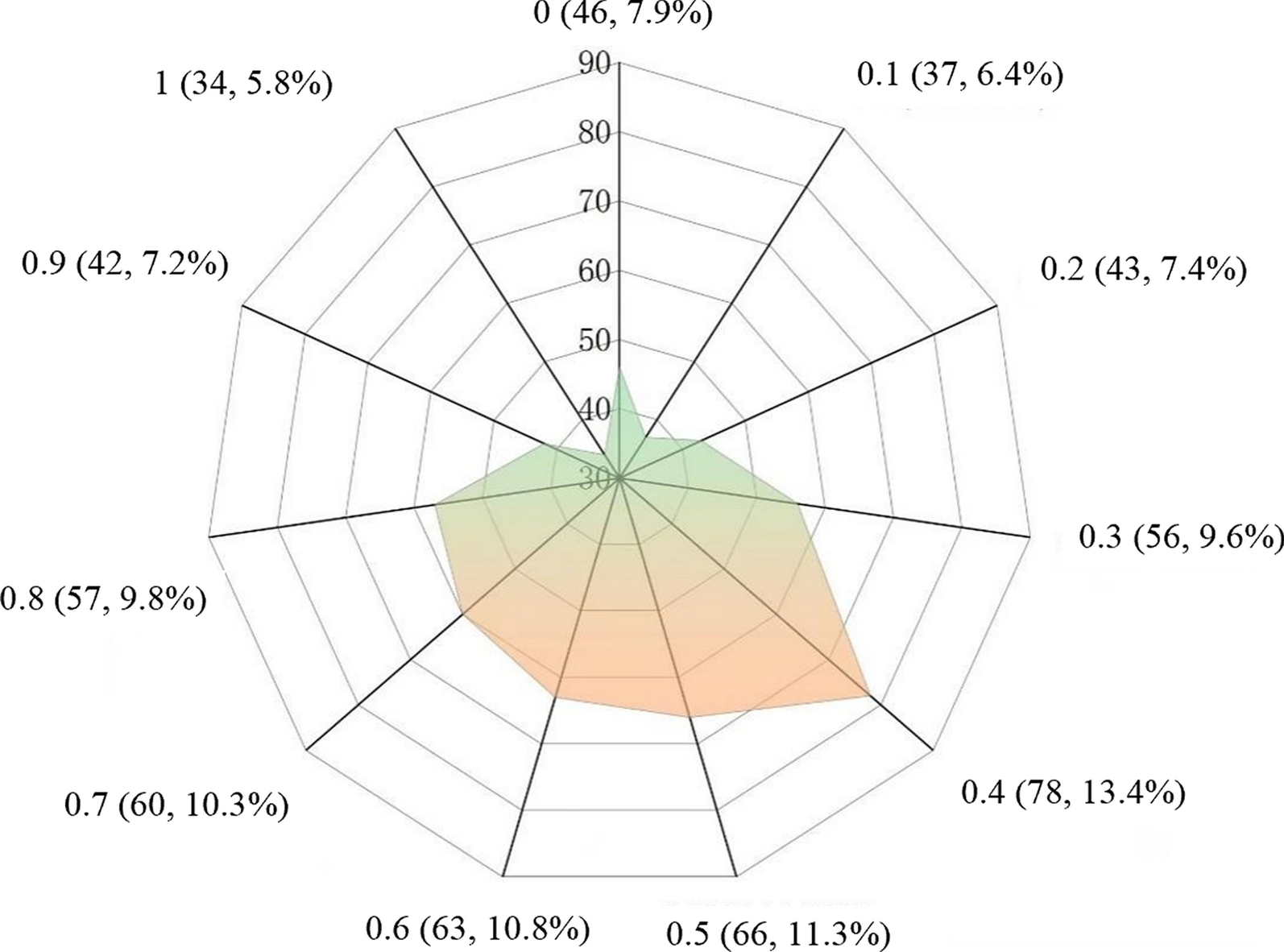
Risk factors for malariaThe GBD 2021 assessed the contributions of three risk factors for malaria-related DALYs. Among these risk factors, the leading risk factor was child underweight, and the second risk factor was child stunting. Globally, the impact of child underweight and child stunting showed a declining trend, whereas the impact of child wasting remained negligible, and 0.14% of DALYs related to malaria were attributed to child underweight, whereas 0.08% of DALYs related to malaria were attributed to child stunting (Fig. 5). In high-SDI regions, the impacts of child underweight and child stunting on malaria DALYs are very small and decrease annually, with child wasting having almost no impact. In high-middle-SDI regions, the impact fluctuated but showed an overall decline, with child underweight having a slightly greater impact than child stunting (Fig. 5A). In the middle-SDI regions, the impacts also showed a declining trend. In the low-middle- and low-SDI regions, the impacts were the greatest, yet they also exhibited a downwards trend (Fig. 5B). Overall, the impacts of child underweight and child stunting on malaria DALYs were greatest in low-SDI regions and minimal in high-SDI regions, with these impacts showing an overall decline from 1990–2021.
Fig. 5
The burden of malaria attributable to risk factors (child stunting, child underweight, and child wasting) across SDI quintiles. A In 1990–2021. B In 2021. SDI: sociodemographic index
留言 (0)