Medication compliance
Drug therapy is the primary treatment option, especially for patients who cannot be treated surgically. Cyst becomes inactive or disappears after 1–2 years of albendazole treatment for CE, and patient compliance affects the long-term treatment outcome [20]. If liver lesions were removed and long-term benzimidazole treatment was used, the survival rates of patients with AE would be comparable to those of healthy people [23]. For patients with AE who cannot be treated with radical surgery, drug chemotherapy has significantly improved the 10-year survival rate from a range of 6.0%–25.0% to a range of 80.0%–85.0% [24].
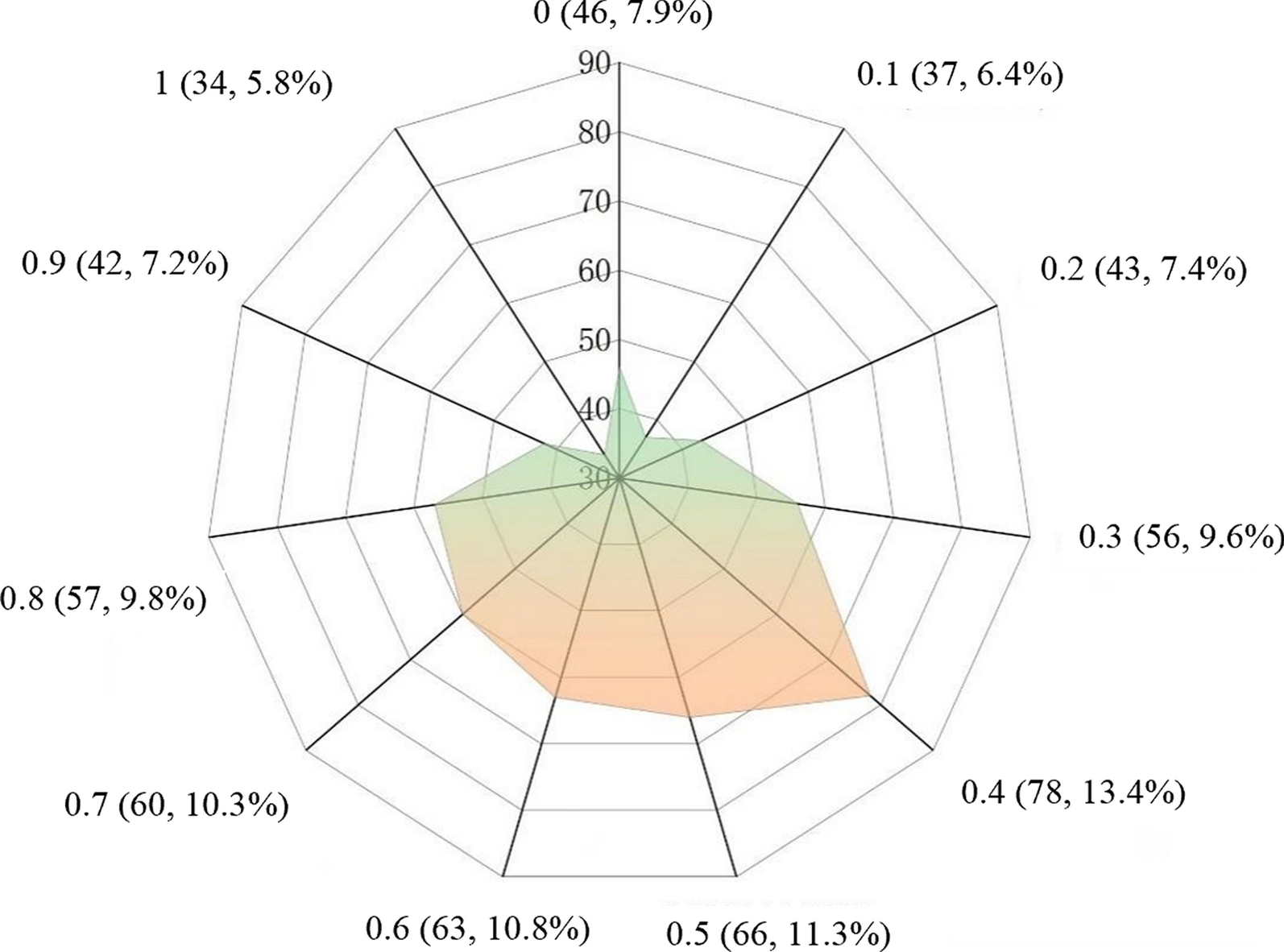
The files of the patients were incomplete, preventing 35.3% of them from being evaluated for medication. These patients might have been lost to follow-up, or their medication information might not have been recorded owing to negligence by follow-up personnel [25]. The medication compliance of the evaluable patients was poor, and 7.9% had never taken albendazole. The majority of patients exhibited satisfactory adherence to medication during the early stages of treatment. However, the medication compliance of patients decreased as a result of the prolonged use of albendazole. Patients with echinococcosis demonstrated poor compliance with albendazole owing to poor knowledge of the disease, albendazole treatment, and adverse reactions [26, 27].
In this study, Tibetans and herdsmen without formal education comprised the majority of patients who failed to comply with medication. Patients with higher education levels, health awareness, and disease cognition are more likely to actively accept drug treatment. Recently, patients with a short course of disease have been diagnosed with echinococcosis, and their symptoms are more noticeable. Their compliance with medication is higher than that of patients with a long course of the disease. Patients with a long course of the disease feel relaxed because they believe their symptoms have improved. Patients with AE demonstrated higher medication compliance than patients with CE because their symptoms were more noticeable, and the disease was more severe. Additionally, the number of patients with AE in this study was small. AE is more complex and severe than CE, requiring long-term or even lifelong medication. This may lead to poor medication adherence among some patients, who may give up taking medication midway. It is important to follow up with these patients and remind them to take medication and undergo follow-up examinations regualarly.
Albendazole emulsion has an unpleasant taste and is unpalatable to some patients. However, it has a higher absorption rate than tablets and can improve treatment effectiveness [28]. We discovered that patients who combined tablets and emulsions exhibited higher compliance, implying that the patients preferred to choose their own suitable dosage form. The occurrence of adverse reactions was the main factor that affected patient medication compliance. The findings revealed that 85.1% of patients experienced mild adverse reactions and needed no treatments. However, 45.9% of patients discontinued taking albendazole owing to adverse reactions, indicating that patients exhibited poor knowledge of adverse reactions. We compared the results with those of other studies. Patients with echinococcosis exhibited poor compliance with albendazole owing to poor knowledge of the disease, albendazole treatment, and adverse reactions, indicating that the patients did not know how to deal with the adverse reactions properly. This suggests that patient health education on adverse reactions should be increased.
Additionally, patients who did not trust or pay attention to albendazole treatment, nor did understand treatment duration, exhibited poor medication compliance. Some Tibetan patients trusted traditional Tibetan medicine more and preferred to take local Tibetan medicine. Additionally, patients with echinococcosis are mainly herdsmen, especially Tibetans, who engage in nomadism [29]. During summer, they may be unable to obtain albendazole when they are nomadic in remote pastures. Consequently, herders have greater difficulty obtaining medications than farmers. Furthermore, Tibetan areas are located on the Qinghai-Tibet Plateau, making transit difficult. Some patients are unable to take albendazole on time because they are away or attending school.
We also suggest that disease control should work with clinical doctors to develop different treatment plans and follow-up times for patients based on their conditions, and judge the patient's medication time based on these indicators. For example, the Tibetan community, especially herdsmen, should be able to appropriately extend their follow-up interval and distribute more doses of medication. At the same time, a treatment group can be established within the nomadic community to supervise each other's medication, and a healthy supervisor can also be set up. After being informed of the characteristics of the two dosage forms, patients select the matching dosage form based on their sensitivity and convenience to avoid waste. Health education needs to focus on introducing the treatment of echinococcosis, especially the characteristics and necessity of drug therapy, as well as the effectiveness of albendazole treatment. It should also be emphasized that the characteristics of the two dosage forms to patients, as well as the possible adverse reactions, symptom manifestations, and treatment methods of albendazole, in order to alleviate patients’ fear of albendazole. Follow up and follow-up examinations are important means of reminding patients to take medication and evaluating the effectiveness of their treatment, which requires their cooperation. In health education, it is also necessary to emphasize the necessity of follow-up and re examination in drug treatment, which is related to their course of treatment.Treatment groups can also be established based on the patient's village or community, and healthcare professionals can be arranged to answer their questions, remind patients to take medication or undergo follow-up examinations. Health education should pay special attention to patients with relatively low levels of education, who may not be familiar with or even have misunderstandings about the treatment of echinococcosis and albendazole drugs, and may not value the importance of follow-up and re examination. These are the key to providing health education to them, and patients who take medication regularly and have good treatment effects can be invited as promoters to educate them.
Medication compliance may vary depending on factors such as disease duration, severity, and type. In this study, patients in ten echinococcosis-endemic counties from three endemic provinces in China were investigated for medication compliance, with good representativeness; however, it did not include all epidemic counties.
Therapeutic efficacy
Cure and effectiveness rates were 5.2% and 32.2%, respectively, which are lower than previously reported data where the cure rate of albendazole treatment for patients was approximately 30.0%, with an effectiveness rate ranging from 40.0% to 60.0% and an inefficacy or recurrence rate of 30.0% [30]. This may be attributed to the fact that only patients with follow-up records within the past year were included in this study, while follow-up information for other patients who were medication-compliant was not documented, making it impossible to evaluate their treatment outcomes. In this study, patients who adhered to regular medication displayed considerably better treatment outcomes than those who did not adhere to medication or did not take medication, consistent with findings from other studies [30, 31]. This implies the need for improved patient health education to enhance medication adherence, as albendazole therapy is a long-term procedure, especially for certain cystic types that remain active. This will increase the disease and economic burden on patients. For patients who cannot undergo surgical treatment, standardized medication is the most cost-effective and only treatment option. Regular medication can improve patient treatment outcomes, indicating that relevant departments should increase the intensity and quality of patient follow-up and health education, ensure effective follow-up work implementation, and improve patient medication adherence to further improve cure rates and quality of life.
In this study, the effectiveness and cure rates for patients who had taken medication for more than 36 months were 40.3% and 9.0%, respectively, which are lower than those reported by Li et al., where the effectiveness rate of albendazole treatment for patients with CE after 3–6 months was 30.0%. When treatment was extended for 18–30 months, the number of cysts decreased by 32.7%, and cystic degeneration decreased by 49.0%, yielding an overall effectiveness rate of 81.0% [30]. Due to its low absorption rate in the intestine and low concentration of active ingredients in the capsule, albendazole requires an increased dosage to achieve therapeutic effects. However, high-dose medication can cause some adverse reactions, leading to poor medication compliance and liver damage, causing additional physical damage and economic burden to patients. The treatment of CE is related to the size, classification, and quantity of the patient's lesions. However, in this study, no stratified analysis was conducted on the characteristics of patient lesions.
A small number of patients obtained follow-up results within the previous year, making it difficult to assess patient treatment outcomes. Therefore, only 174 patients were evaluated for treatment effectiveness, reflecting the problems in the management of patients with CE medication treatment as well as poor compliance and a lack of emphasis on follow-up.
Suggestions
We recommend the following: First, relevant departments must improve the quality of patient management and record-keeping. Second, it is necessary to focus on patient health education to increase their knowledge of the disease, treatment, and reexamination, especially the performance and treatment of albendazole-related adverse reactions, to reduce the fear of adverse reactions. Drug therapy is a long-term procedure that requires patients to regularly re-examine and evaluate its efficacy. Third, follow-up personnel should receive more professional and comprehensive training, and they should be required to fully document each follow-up. Albendazole must be dispensed in a flexible manner. After being informed of the characteristics of the two dosage forms, patients select the matching dosage form based on their sensitivity and convenience to avoid waste. Regarding patient nomadism, follow-up personnel should keep open communication with patients, regularly assess the existing albendazole stock of patients, leave a buffer time for drug distribution, and avoid the situation of insufficient drugs for patients.
More extensive and diversified health education and professional guidance should be provided to patients receiving medical treatment in community health services to improve their knowledge of the harm caused by echinococcosis, albendazole treatment of echinococcosis, adverse reactions, and follow-up management, thereby increasing their trust and confidence in albendazole treatment and alleviating their fear of adverse reactions. Their families and community doctors and officials should be invited to attend. Actively implementing regular management for patients with echinococcosis undergoing medication therapy can increase their adherence to regular treatment, as well as delay and prevent progression and recurrence. Tertiary prevention can increase cure rates, decrease disability and mortality rates, and improve their quality of life.In this study, the medical files of some patients might not have documented timely information about their albendazole use. Additionally, some patients might have had recall bias during the investigation, resulting in an underestimation of medication compliance.
Limitations
The limitations of this study include a sample size and a large number of excluded cases. First, 35.3% of the research patients corresponding to the files were excluded from the analysis, which could have resulted in selection bias that could not be evaluated. Second, surveying 10 out of the 370 endemic counties in China resulted in low representativeness. Third, in the analysis of the treatment effect of CE patients, the inclusion of too few patients may lead to selection bias and cannot represent the actual treatment situation of patients. These biases can lead to discrepancies between research results and actual situations. In future research, we recommend conducting long-term follow-up on patients to obtain more accurate information on their medication use and treatment outcomes. Additionally, it is recommended to include more patients in future analyses. There may be differences in health education strategies in different regions. Therefore, we aim to conduct a uniform nationwide special survey in the future.







留言 (0)