
記住我

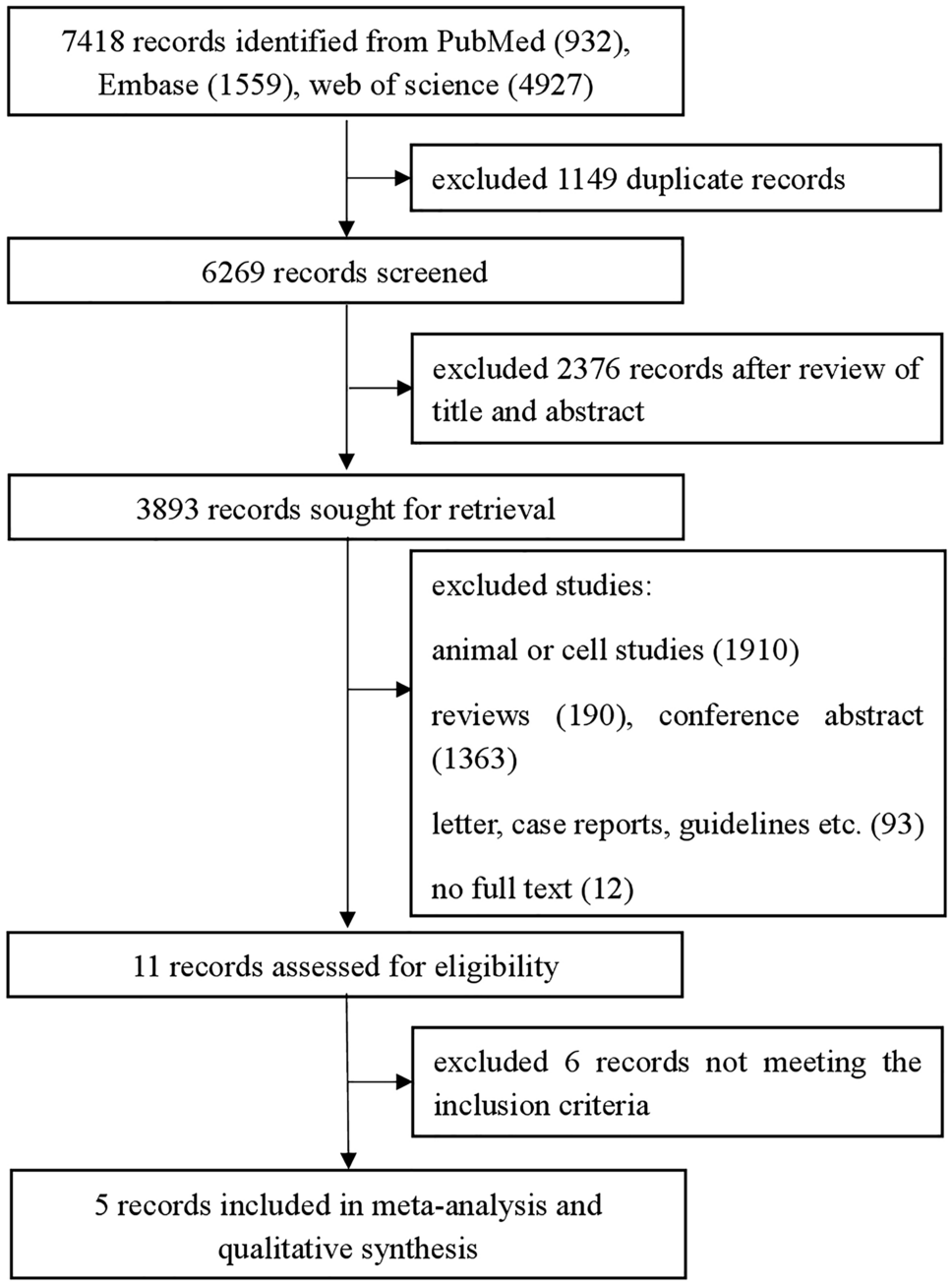

This multicenter, retrospective study included consecutive patients with liver malignancy intended for curative hepatectomy who received preoperative PVE. Patients were included from three Swedish medical centers, i.e., Karolinska University Hospital (center 1), Linköping University Hospital (center 2), and Skåne University Hospital Lund (center 3), between January 2013 and December 2021. Patients were excluded if they had: (1) left-sided PVE, (2) no imaging evaluation after PVE, (3) PVE plus hepatic vein embolization, (4) PVE after associated liver partition and portal vein ligation for staged hepatectomy (ALPPS) stage 1, and (5) no available pretreatment CT scans were obtained at portal venous phase. The patient selection process and the study workflow are shown in Fig. 1.
Fig. 1
Patient selection process (A) and the prediction model building workflow (B). ALPPS, associating liver partition and portal vein ligation for staged hepatectomy; PVE, portal vein embolization; HVE, hepatic vein embolization
At each participating center, the decision to conduct PVE was determined by a multidiscipline tumor team, which comprehensively assessed pretreatment standardized FLR (pre-sFLR), the patient’s medical history and treatment history. For patients who had undergone chemotherapy, the pre-sFLR threshold was adjusted to 30%. In cases where patients had cirrhosis, the pre-sFLR threshold was established at 40%.14 The details of the PVE procedure have been described in previous work.15
According to our statistical power analysis, at least 100 patients were required to develop a prediction model achieving an AUC > 0.7 with a significance level (α) of 0.05 and a statistical power (1–β) of 0.90 when assuming an incidence of insufficient FLR hypertrophy of 30%. The insufficient FLR hypertrophy rate (30%) was based on literature and observational data.4,16 The significant difference in AUC between the models was set at 0.1. In this study, center 1 was used for model development (i.e., “derivation cohort”) and centers 2 and 3 for model performance evaluation (i.e., “external test cohorts”). During the process of model development, test cohorts were kept blind.
This study was approved by the Swedish Ethical Review Authority with approval number Dnr: 2019-01297. Informed consent was waived due to the retrospective nature of the study design. Patient information and image data were deidentified and analyzed in an anonymized manner.
Clinical Factors and Liver Volume CalculationPatient clinical data at baseline (prior to PVE) were retrieved from the hospital electronic records, including demographic information, body mass index (BMI), overall physical performance, chronic diseases, diagnosis, history of chemotherapy, laboratory tests (usually obtained the day before PVE), liver function evaluation, and PVE procedure-related information, such as embolization method and materials. For clinical variables with a missing rate ≤ 5%, the missing value was imputed by median for continuous variables and mode for categorical variables; variables with missing rate > 5% were abandoned.
Liver volume was calculated based on radiological imaging such as CT or MRI before and after PVE, according to local practice. The sFLR was determined by dividing the radiologically measured FLR with the estimated total liver volume, following the formula proposed by Vauthey:17 estimated total liver volume = − 794.41 + 1267.28 × body surface area. The body surface area was calculated using Mosteller’s formula.18 Kinetic growth rate (KGR) was determined as (post-sFLR-pre-sFLR)/time elapsed in weeks.
In this study, insufficient FLR hypertrophy was defined as post-sFLR < 30% after PVE at first imaging evaluation, considering that a majority of patients had undergone previous chemotherapy, and in the case of concomitant cirrhosis, a post-sFLR cutoff of 40% was applied.
Clinical Model DevelopmentUnivariable logistic regression analysis was performed on clinical factors to detect the associations between them and FLR hypertrophy. Clinical factors with p < 0.1 were subjected to multivariable logistic regression analysis. The Akaike information criterion was employed to determine the number of predictors kept in the model. The clinical model was constructed by linear combination of these variables weighted by the corresponding coefficients.
Radiomics Signature DevelopmentCT Scan Acquisition and FLR SegmentationPortal venous phase images of iodinated contrast-enhanced CT before PVE treatment were selected for radiomics analysis in this study. The scanning and reconstruction parameters included: tube voltage ranging from 70 to 120 kVp, tube current between 120 and 300 mAs, a pitch varying from 0.6 to 1.25 mm, an image matrix of 512 × 512, and a reconstruction slice thickness of 0.6–5 mm.
As the CT images stemmed from different centers with various manufacturers and scanning protocols, imaging preprocessing was performed to standardize the images. The image voxel size was re-sampled to 1 × 1 × 1 mm3 by the B-spline approach and the intensity histogram was discretized using a fixed bin width of 25. After that, the FLR was manually segmented by one researcher (Q.W. with 6 years of abdominal imaging) at the portal vein bifurcation level of the cross-section CT image, by using ITK-SNAP (version 3.6.0) (Fig. 2). To evaluate reproducibility of radiomics features, 20 patients were randomly selected from the derivation cohort and delineated by another independent researcher. The interclass correlation coefficient (ICC) was calculated.
Fig. 2
A representative case of CT study. A Radiomics features were extracted from the segmented future liver remnant part at the slice of the bifurcation level of the main portal vein. B Four representative radiomics features that show a texture pattern different from that perceived by human naked eye
Radiomics Feature ExtractionRadiomics features were extracted from the segmented FLR by using the Python-based library pyradiomics (version 3.1.0). The following categories of radiomics features were extracted: shape, first order, gray level co-occurrence matrix, gray level dependence matrix, gray level run length matrix, gray level size zone matrix, and neighborhood gray tone difference matrix (Supplementary Table S1). The definitions of the radiomics features are available at https://pyradiomics.readthedocs.io/en/latest/features.html.
Radiomics Feature SelectionAs the extracted radiomics features were high dimensional, feature selection was conducted to reduce potential overfitting when developing the model. Specifically, a “three-step” strategy was adopted: (1) radiomics features with ICC > 0.80 were selected, (2) Spearman correlation analysis between any two radiomics features was performed to compare the similarity of each feature pair (if the coefficient of the feature pair was larger than 0.95, one of them was randomly removed), and (3) Spearman correlation analysis was further conducted to evaluate the association between radiomics features and liver growth rate (i.e., KGR), and the significant radiomics features (p < 0.05) were chosen. With this “three-step” strategy, reproducible, non-redundant, and clinically significant radiomics features were chosen.
Radiomic Signature ConstructionThe radiomics features were normalized by Z-score before developing the radiomics signature. The Kruskal–Wallis test was performed, and the features were sorted by their
F-values. Support vector machine (SVM) was applied to develop the radiomics signature. The linear kernel function was adopted as it has good interpretability of the final model. To achieve a balanced classification between positive and negative samples, the synthetic minority oversampling technique (SMOTE) was adopted.19 To determine the hyperparameters of the model, a fivefold cross-validation was applied in the derivation cohort. The predicted probability was used as the FLR radiomics signature.
Construction of Combined ModelThe developed radiomics signature was incorporated into the clinical model to build a combined clinical–radiomics model. The performance of the combined model was evaluated and compared with the clinical model in both derivation and test cohorts.
Statistical AnalysisContinuous variables are expressed as mean and standard deviation when the data was normally distributed and compared by Student’s t-test; when nonnormally distributed, they were expressed as median with interquartile range and compared by the Mann–Whitney U test. Categorical variables were presented as number and percentage and compared using chi-squired test or Fisher’s exact test.
The discriminative ability of the models was evaluated by the area under the curve (AUC), accuracy, sensitivity, specificity, and positive and negative predictive values. The calibration ability of the model was intuitively visualized by a calibration curve. The optimal threshold was determined by Youden’s index, which maximizes the sum of sensitivity and specificity. This optimal threshold of the combined model was also applied for patient risk stratification (low/high-risk group). A two-tailed p value less than 0.05 was regarded statistically significant. Statistical analysis and data visualization were conducted by using R software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria) with corresponding packages. Sample size was estimated using PASS software (version 15.0.5; Utah, USA).
留言 (0)