
記住我



This retrospective study included consecutive patients diagnosed with complex renal cysts who underwent renal cyst unroofing, nephron-sparing surgery and radical nephrectomy from January 2010 to December 2019. This study protocol was approved by the ethics committee of our hospital (IRB00006761-M2022169).
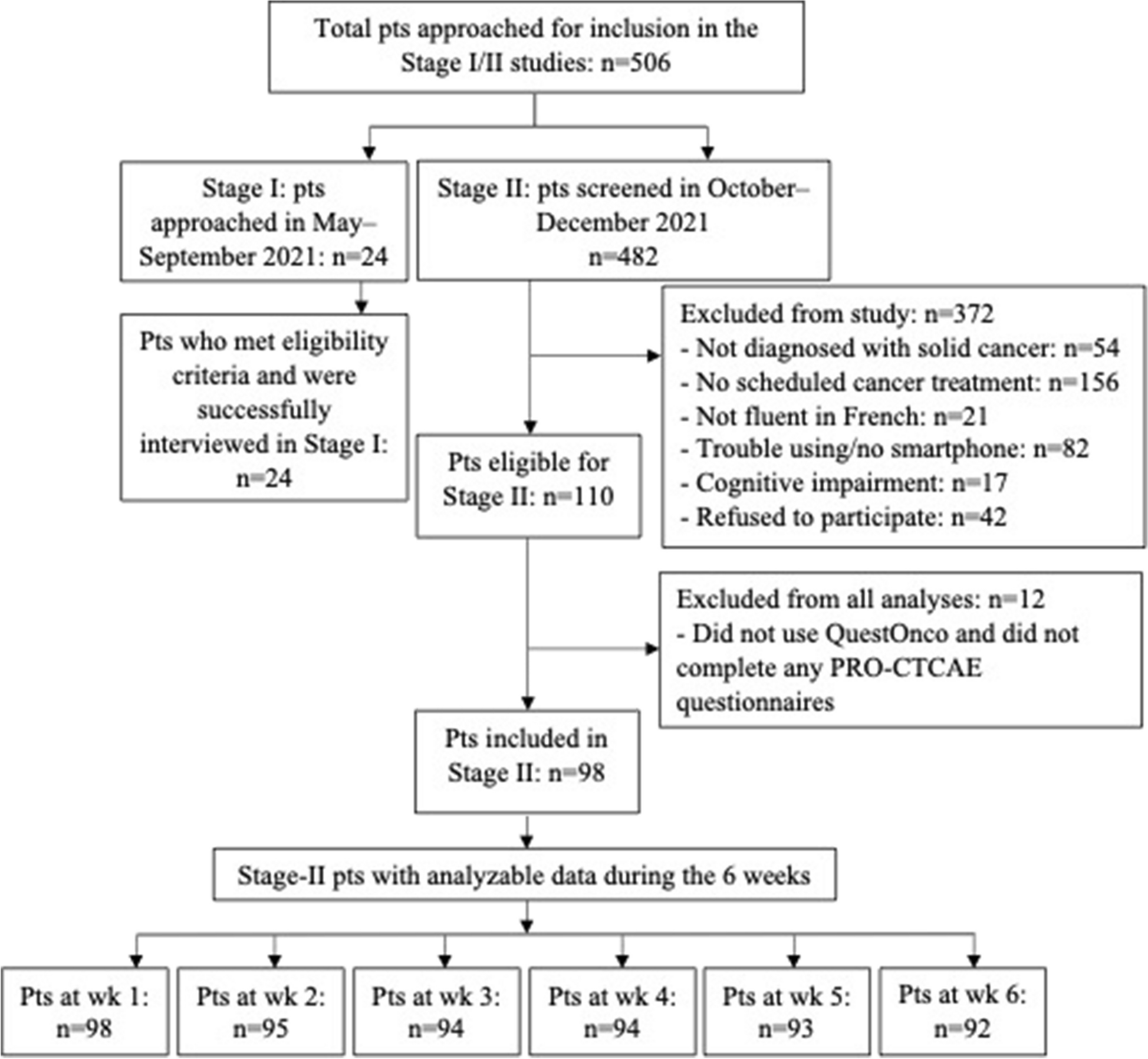
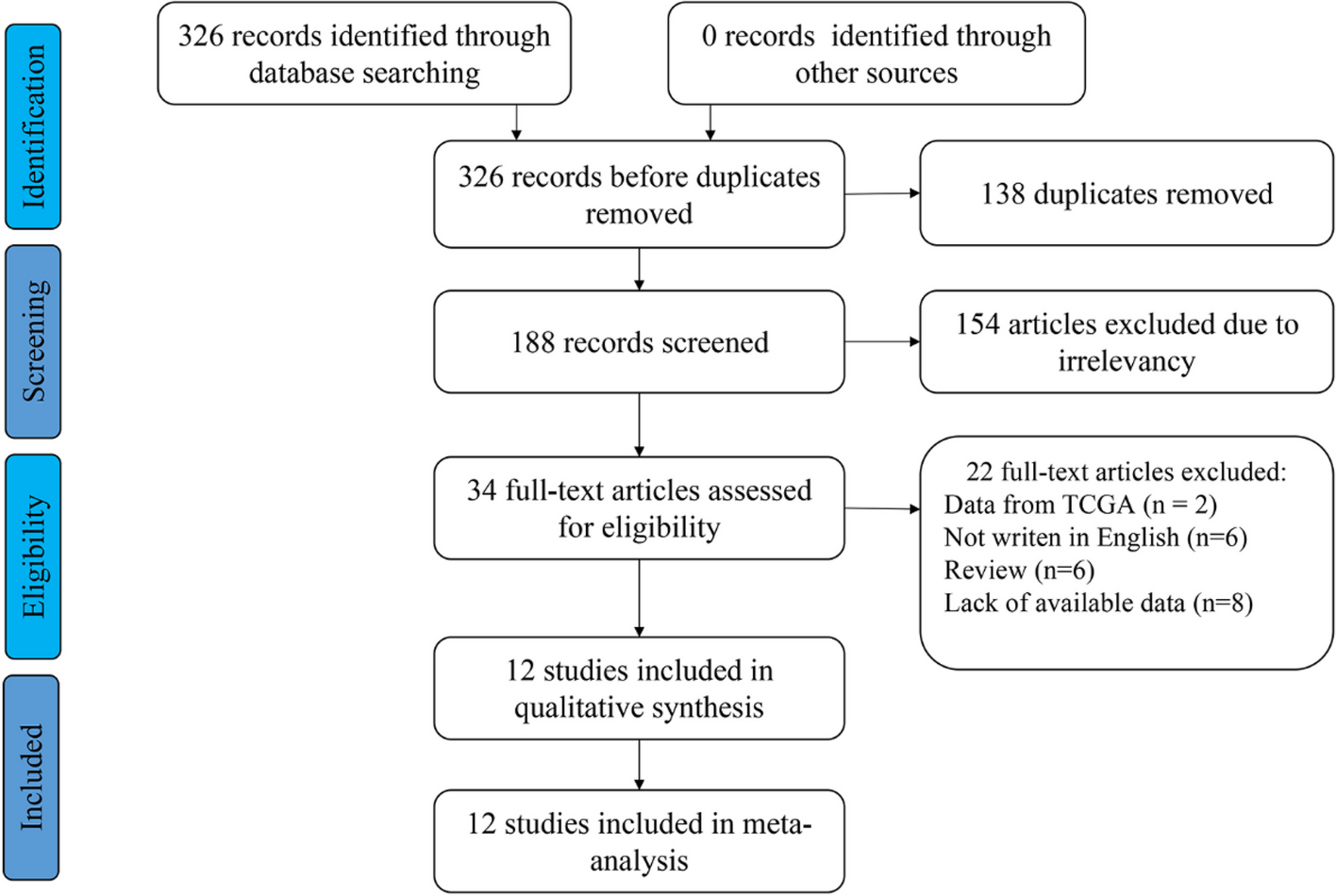
The inclusion criteria were as follows: (1) unenhanced and cortical CT images acquired within 2 weeks before surgery; (2) Bosniak II-IV cysts; and (3) completed surgery with definite postoperative pathology. The exclusion criteria were as follows: (1) incomplete medical records; (2) low-quality CT images; and (3) Bosniak I cysts. Pathology was based on the 2016 WHO classification of renal cell carcinoma and reviewed by two experienced pathologists [11]. The flowchart on the patient selection and study design were shown in Supplementary Materials 1.
A total of 322 patients were ultimately included in the study. The patients were randomly divided into 4 sets for 4-fold cross-validation. During the feature selection and model construction in each fold, three sets were used as a training set, and one set was used as a testing set. Each testing set was totally independent from each training set. Additionally, subgroup analysis was performed in 82 patients with Bosniak IIF-III cysts.
Bosniak classificationThe Bosniak classification used in this study was based on the updated Bosniak classification of 2019 [6], which was evaluated and reviewed by experienced radiologists and urologists. Examples of Bosniak I-IV cysts are shown in Fig. 1.
Fig. 1
Examples of Bosniak I-IV cysts. A: Bosniak I; B: Bosniak II; C: Bosniak IIF; D: Bosniak III; E Bosniak IV
CT acquisitionAbdominal contrast-enhanced CT scans were obtained from all participants using a 64-slice scanner (GE Discovery HD 750, GE Healthcare). The participants were asked to abstain from food for 6–8 h prior to the examination. The fixed acquisition parameters were as follows: 120 kV, automatic tube current modulation technique; detector collimation: 64 × 0.625 mm; matrix: 512 × 512; reconstruction slice thickness: 5 mm; and standard convolution kernel. Nonionic contrast medium (iopromide, Ultravist 370 mg/mL; Bayer) was intravenously administered at a dose of 1.5 mL/kg body weight and a rate of 3 mL/s. The scan was sequenced into three phases, namely, the cortical, medullary, and excretory phases, which were initiated at 12, 37, and 170 s after injection, respectively.
SegmentationDigital Imaging and Communications in Medicine (DICOM) images were exported from the picture archiving and communication system (PACS) after desensitization. The segmentation of the cysts was performed by a resident with 3 years of experience and confirmed by a professor with 30 years of experience via ITK-Snap (version 3.8.0). A fully manual slice-by-slice segmentation was performed without the use of any threshold or semiautomatic tools. The segmentation was guided by the following principles: (1) All segmentations were executed on the axial plane, progressing slice by slice from the initial to the final cyst image to delineate the volume of interest (VOI). (2) Segmentation was performed along the edge of the cyst as much as possible. (3) The cortical images served as a reference for the unenhanced scan images, with an effort to ensure consistency between the segmentation areas of unenhanced and cortical CT scans.
Radiomics feature extractionRadiomics features were extracted from both the original CT images and the transformed CT images with the PyRadiomics 3.0.1 package. The extracted features are similar to those used in our previous research [12]. In total, 1334 features were extracted from each patient. The calculation feature list is presented in Supplementary Table 1.
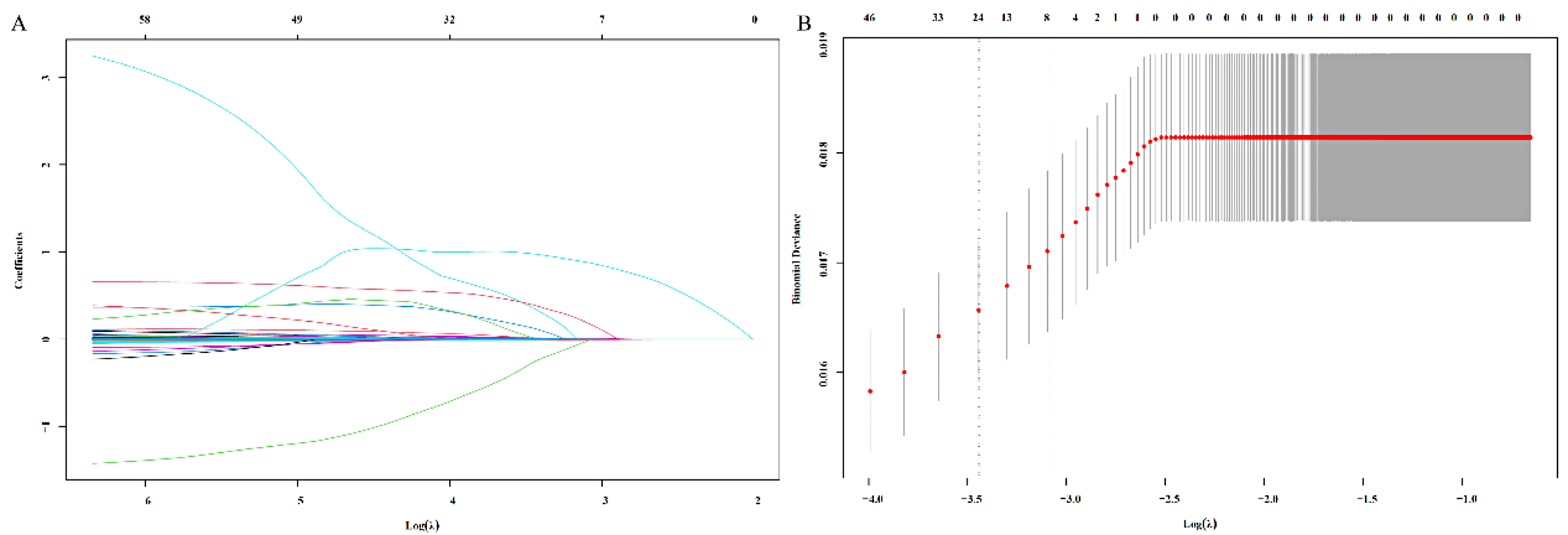
Feature selection and model constructionBefore feature selection, the z-score normalization was used to normalize the radiomics features of training set and then transform those of the testing set. Then least absolute shrinkage and selection operator (LASSO) regression was subsequently used for feature selection. The LassoCV function from scikit-learn (version 1.0.1) was implemented for lasso feature selection. The lambda value of LASSO model was selected from a geometric sequence which contained 50 numbers on a range of [10 − 3, 103]. The selected lambda value was shown in Supplementary Materials 2. The Lasso model was optimized using leave-one-out-cross-validation (LOOCV) on the training dataset. Logistic regression (LR), support vector machine (SVM) and random forest (RF) models were constructed. The construction of the models was performed with the Scikit-Learn 1.0.1 package. A grid search method was used to select the best hyperparameters of the machine learning models in this study. For the optimization of LR models, a grid search approach with 5-fold cross-validation on the training set was applied for selecting the optimal C from 2i, where i was an integer from the range of [-8, 11]. For the optimization of SVM models, a grid search approach with 5-fold cross-validation on the training set was applied for selecting the optimal C from a geometric sequence which contained 10 numbers on a range of [2 − 1, 23], and gamma from a geometric sequence which contained 50 numbers on a range of [2–4, 2]. For the optimization of RF models, a grid search approach with 5-fold cross-validation on the training set was applied for selecting the optimal estimator from , criterion from , max features from , max depth from , and min samples split from . The selected hyperparameters of the models can be seen in Supplementary Materials 2. The accuracy, sensitivity, specificity and area under the receiver operating characteristic curve (AUC) of the models were calculated separately.
Statistical analysisStatistical analysis was performed with SPSS version 24.0 and Python version 3.8. For clinical data, categorical variables were analysed via the chi-square test, and continuous variables were analysed via the t test or Mann‒Whitney U test. The average AUC, accuracy, sensitivity, and specificity of each model were calculated to assess the diagnostic efficacy of the model. The AUC, accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) with 95% confidence intervals (CI) were provided. A two-tailed P value < 0.05 was considered to indicate statistical significance.
留言 (0)