
記住我


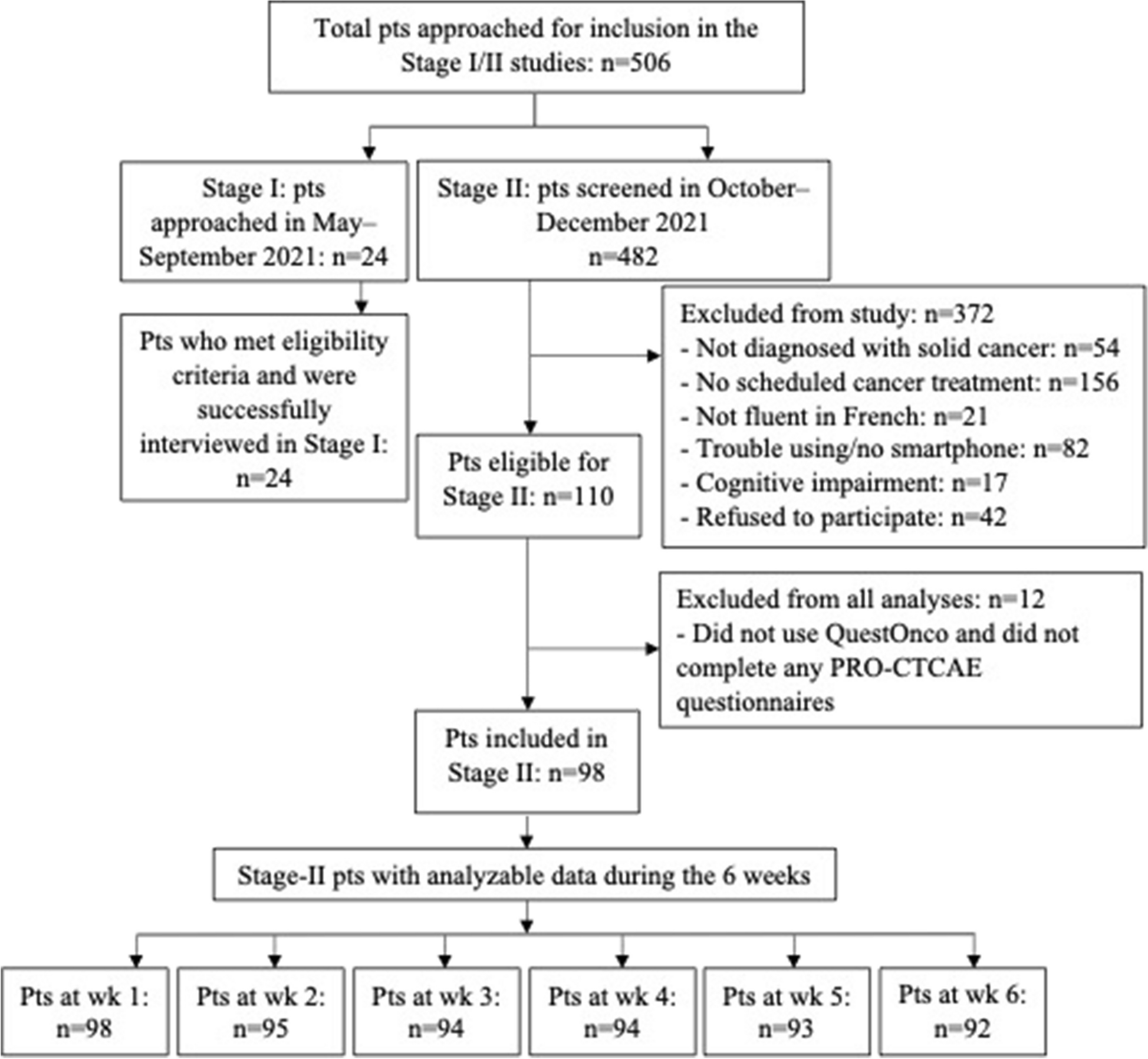
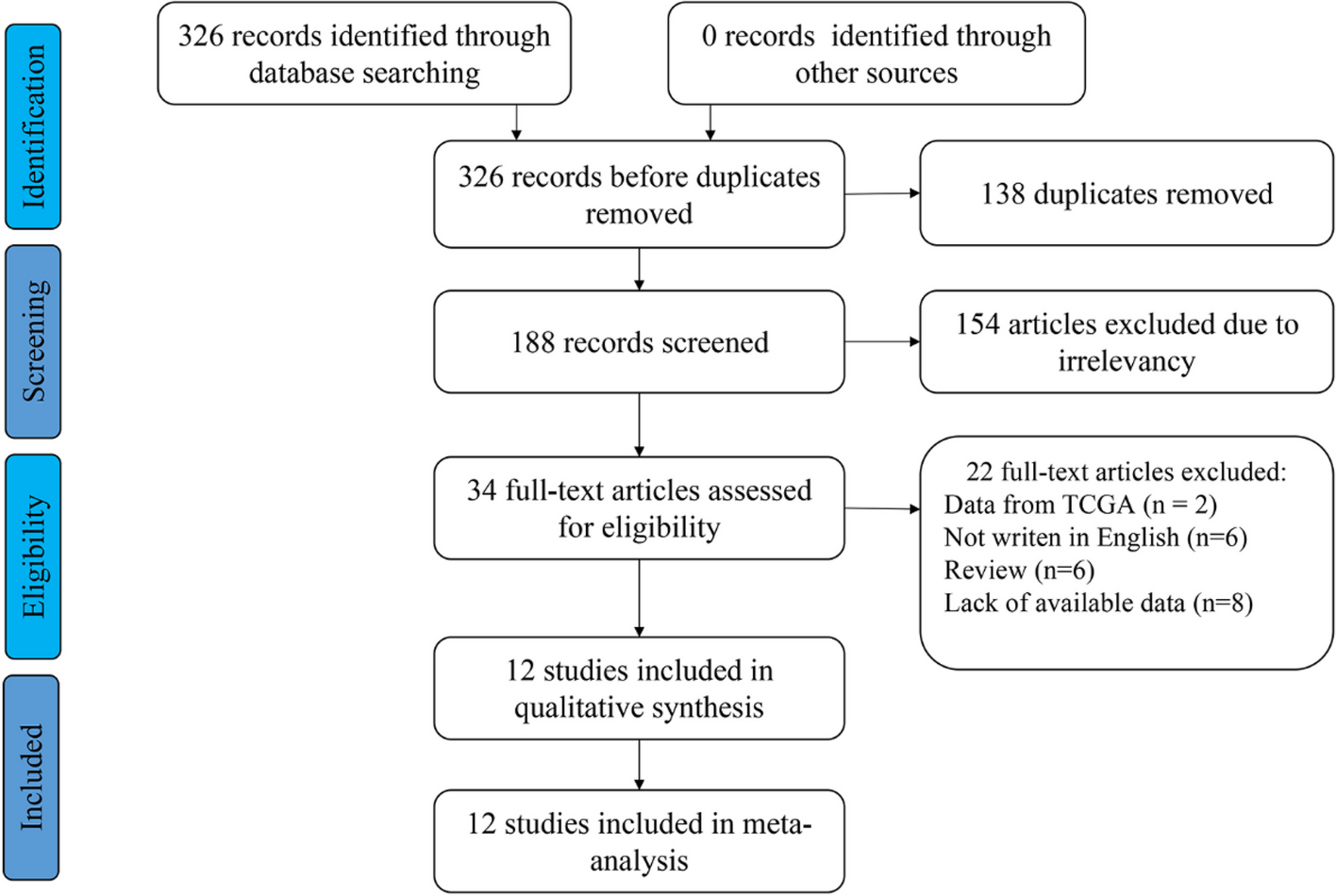

A total of 4,918 citations were identified in the initial search. After removing duplicates, 4,380 studies remained. Following the screening of titles and abstracts, 4,290 studies were excluded due to inconsistency in study types, irrelevance to the topic, or ineligible populations. Upon reviewing the full texts of the remaining 90 studies, 61 were subsequently removed. One study was supplemented by a snowballing search. The quality of the remaining 30 studies was assessed, leading to the exclusion of 15 studies that were rated as having a high risk of bias. Ultimately, 15 studies were included, comprising 7 RCTs rated as low risk for bias and 6 RCTs rated as some concern of bias, and 2 quasi-experimental studies rated as low risk or moderate risk of bias. The PRISMA flow chart illustrating this process is shown in Fig. 1.
Fig. 1
Flow diagram of the study selection
Study characteristicsThe 15 studies included in this review were published between 2011 and 2024, with 60% (n = 9) appearing in the last five years (2020 to 2024). The majority of studies employed an RCT design (n = 13, 87%). Eight studies were conducted in mainland China, two in the Hong Kong Special Administrative Region of China, two in England, and the remaining three in Vietnam, Thailand, and Taiwan, China. Five of the studies were conducted in outpatient settings, including radiotherapy outpatient clinics, oncology and respiratory medicine outpatient clinics, as well as psychological nursing clinics. Twelve were single-centre studies and the remaining three were multi-site studies.
Furthermore, the 15 included studies encompassed a total of 1,692 participants, with sample sizes ranging from 30 to 263. The average age of the participants varied, ranging from 45.15 (SD = 4.34) to 69.5 (SD = 10.20) years. The majority of participants had advanced-stage lung cancer (stage III or IV). In terms of treatment methods, chemotherapy was the most commonly adopted approach, followed by surgery and radiotherapy. Further details about the characteristics of the included studies can be found in Table 1.
Table 1 Characteristics of the included studiesIntervention characteristicsNine studies employed individual interventions, two utilized group interventions, and the remaining four employed a combination of both individual and group approaches. With respect to interventionists, eight studies (53%) exclusively utilized nurses, whereas the other studies involved professional athletic coaches or multidisciplinary teams. The minimum duration of intervention was one-week, whereas the maximum duration spanned six-months. The frequency of interventions ranged from two to 36 sessions. Six studies followed patients for varying durations, ranging from 3 weeks to 9 months after the intervention. All studies employed face-to-face interventions, with approximately 86% (n = 12) incorporating telephone follow-ups and 29% (n = 4) utilizing the WeChat platform for communication. Five studies designed interventions based on established theories, models, or frameworks. For instance, Khamboon and Pakanta [15], and Li et al. [35] developed cognitive-behavioural intervention programs utilizing Symptom Management Theory and Ellis's “ABC” theory, respectively. Chan et al. [31] devised an analytical model to elucidate the connection between psychoeducational interventions and their outcomes. Yorke et al. [32, 33] applied the Medical Research Council framework to create and assess complex interventions. The full intervention characteristics of the studies included in this review are detailed in Table 2.
Table 2 Intervention characteristics of the included studiesWe classified the interventions in the study into five groups: a) Educational interventions—encompassed psychoeducational interventions and medication health education based on the Multinational Association for Supportive Care in Cancer Oral Agent Teaching Tool (MOATT) [37]; b) Exercise interventions—home-based walking, aerobic exercise, tai chi, and qigong training. c) Psychological interventions—cognitive-behavioural interventions and narrative care; d) Multimodal interventions—combine two or more approaches, as exemplified by the respiratory distress symptoms intervention programme developed by Yorke et al. [33], which incorporates breath control, cough suppression, acupressure, and exercise; and e) Complementary or alternative medicine (CAM) interventions—specifically involving auricular acupressure therapy and acupuncture.
Effectiveness of the intervention on symptom cluster/outcomeAs depicted in Table 3 and Fig. 2, we categorized symptom clusters into physiological, psychological, and psychosomatic dimensions. The most frequently assessed symptom clusters were pain-fatigue-sleep disturbance (n = 4), anxiety-depression (n = 4), and breathlessness-fatigue-anxiety (n = 2). Additionally, individual symptoms and other outcomes, such as QOL and functional ability, were assessed using scales or questionnaires. In the included studies, outcomes were measured initially before the intervention (baseline), and subsequently one or more times after the intervention, with two to four assessments in total. The most common time point for follow-up surveys was at the end of the intervention (n = 15), followed by two months (n = 2) and three months (n = 2) after completion of the intervention.
Table 3 Effectiveness of the different intervention typesFig. 2
Effectiveness of the different interventions Note: ( +) = Statistically significant; ( −) = Not statistically significant; * denotes that the symptom cluster was examined most frequently in the included studies; CAM, complementary or alternative medicine; MOATT, Multinational Association for Supportive Care in Cancer Oral Agent Teaching Tool
Educational interventionTwo studies [31, 37] reported that the educational interventions had a positive effect on the management of the breathlessness-fatigue-anxiety symptom cluster in lung cancer patients. Moderate to substantial effects of the intervention were observed for this symptom cluster (Cohen's d ranged from 0.47 to 1.03), and positive effects persisted for three weeks and nine weeks after the intervention. Among single symptoms, the most significant post-intervention improvement was observed for nausea (Cohen's d = 2.19), followed by distress (Cohen's d = 1.76) and then pain (Cohen's d = 1.44). Furthermore, the educational intervention resulted in a significant improvement in functional ability that lasted for nine weeks after the intervention (Cohen's d ranged from 0.09 to 0.46).
Exercise interventionIn three studies [18,19,20], exercise interventions were primarily employed to manage the sleep disturbance-anxiety-depression-fatigue symptom cluster and the breathlessness-fatigue-anxiety symptom cluster. However, no significant improvement was observed in these symptom clusters post-intervention. With respect to individual symptoms, the findings were mixed. One study found that an exercise intervention had a moderate effect on the improvement of anxiety and depression that lasted for three months (Cohen's d ranged from 0.19 to 0.63), but the impact on physical symptoms was insignificant (p > 0.05). Conversely, another study reported a notable improvement in cough following a six-week follow-up (p < 0.05). Additionally, there were significant enhancements in global health, functional health, and symptom-related QOL at six weeks post-intervention (p < 0.05).
Psychological interventionAll three studies included [15, 16, 35] demonstrated favorable effects of psychological interventions on the following symptom clusters: fatigue-loss of appetite-anxiety cluster (Cohen's d from 1.49 to 1.55), pain-insomnia-fatigue cluster (Cohen's d ranged from 1.32 to 1.84), and anxiety-depression-pain-sleep disturbance symptom cluster (Cohen's d ranged from 0.59 to 0.83). However, the sustained effects of these intervention have not been reported. In terms of individual symptoms, psychological interventions have been reported to have a strong effect on alleviating anxiety and depression in lung cancer patients (Cohen's d = 1.85 and 1.96, respectively). Additionally, patients who received psychological interventions experienced a shorter length of stay (Cohen's d = 1.16) and reported better mood states (Cohen's d = 0.52) than did those in the control group.
Multimodal interventionAmong the five multimodal interventions [17, 32, 33, 36, 38], two studies reported significant improvements in the fatigue-pain-sleep disturbance symptom cluster, with substantial effect sizes (Cohen's d ranging from 0.60 to 2.05). However, the effects on the breathlessness-cough-fatigue symptom cluster were mixed; one study reported a large effect of the multimodal intervention (Cohen's d ranging from 1.79 to 4.68), whereas the other study reported insignificant findings. With respect to individual symptoms, the multimodal intervention was found to be significant for only half of the 16 symptoms evaluated. In terms of effect size, the top three symptoms were lack of appetite (Cohen's d = 1.34) and distress (Cohen's d = 0.79), followed by sleep disturbance (Cohen's d = 0.70). Furthermore, mixed findings regarding anxiety, depression, and QOL have been reported.
CAM interventionOnly two of the studies included in this review utilized a CAM intervention. Jiang et al. [34] used auricular acupressure therapy, which targets symptom clusters, including respiratory, pain-fatigue-sleep disturbance, psychological and emotional, gastrointestinal, and neurological symptom clusters. The study demonstrated significant improvement in all five symptom clusters and in QOL (Cohen's d = 1.17) within the intervention group, with a statistically significant difference from the control group. In addition, Zhang et al. [39] verified the efficacy of acupuncture on a cough-related symptom cluster, and the results showed that acupuncture could relieve the cough of lung cancer patients but did not relieve expectoration or shortness of breath. However, the specific effects of CAM interventions remain unclear due to the absence of similar studies at this time.
Effectiveness of interventions on single symptomsIn this review, meta-analyses were conducted to explore the effects of non-pharmacological interventions on individual symptoms. The outcome indicators were centred on the four most frequently mentioned symptoms in the studies: fatigue (n = 10), anxiety (n = 6), sleep disturbance (n = 5), and depression (n = 5). Importantly, the CAM intervention study was not included in the meta-analysis because of a lack of single symptom scores.
FatigueThe synthesis of ten studies, involving a total of 878 patients, demonstrated statistically significant effects of the non-pharmacological interventions on fatigue (SMD = -1.76, 95% CI [-2.56, -0.97], p < 0.01; see Fig. 3). A random-effects model was applied because statistically significant heterogeneity was observed (I2 = 85%). Sensitivity analyses indicated that excluding any of the studies did not substantially decrease the overall heterogeneity. Subgroup analyses revealed that different types of non-pharmacological interventions had varying effects on fatigue. Specifically, only the educational intervention subgroup [31, 37] exhibited low heterogeneity and proved effective in improving fatigue (SMD = -0.81, 95% CI [-1.23, -0.39], p < 0.01, I2 = 0%; refer to Appendix 4). Among the ten included studies, no statistical (Egger's test, p = 0.916) or visual (Fig. 4) evidence of publication bias was detected.
Fig. 3
Forest plot of non-pharmacological interventions on fatigue
Fig. 4 Anxiety
AnxietySix studies, encompassing a total of 698 patients, investigated the effects of non-pharmacological interventions on anxiety. The meta-analysis revealed a statistically significant effect (SMD = -1.91, 95% CI [-3.04, -0.78], p < 0.01; see Fig. 5). Given the high heterogeneity (I2 = 76%), a random-effects model was employed. Sensitivity analysis indicated that excluding any single study did not substantially alter the pooled heterogeneity. Subgroup analysis revealed that although psychological interventions were effective in alleviating anxiety, heterogeneity persisted (SMD = -3.19, 95% CI [-5.02, -1.37], p < 0.01, I2 = 89%; refer to Appendix 5).
Fig. 5
Forest plot of non-pharmacological interventions on anxiety
Sleep sisturbanceThe meta-analysis of sleep disturbance included five studies involving 424 lung cancer patients. The results revealed statistically significant effects of the non-pharmacological interventions (SMD = -1.36, 95% CI [-1.90, -0.82], p < 0.01; see Fig. 6). Given the presence of statistically significant heterogeneity (I2 = 82%), a random-effects model was employed. In the sensitivity analysis, excluding any single study did not substantially modify the overall heterogeneity. Subsequent subgroup analyses were performed to explore the effects of different non-pharmacological interventions on sleep disturbance. Nevertheless, both the psychological intervention subgroup and the multimodal intervention subgroup retained significant heterogeneity (I2 = 78% and 92%, respectively; see Appendix 6).
Fig. 6
Forest plot of non-pharmacological interventions on sleep disturbance
DepressionFive studies, involving 438 patients, investigated the impact of non-pharmacological interventions on depression. The results demonstrated statistically significant effects (SMD = -2.07, 95% CI [-3.73, -0.40], p < 0.01; see Fig. 7a). Owing to the presence of statistically significant heterogeneity (I2 = 78%), a random-effects model was employed. To assess the influence of individual studies on heterogeneity, a sensitivity analysis was conducted by sequentially excluding each study. After excluding the study by Li et al. [35], the remaining four studies exhibited acceptable heterogeneity (I2 = 0%). Consequently, a fixed-effects model was utilized. Pooled effects indicated that non-pharmacological interventions had a positive impact on depression compared with the control conditions (SMD = -1.48, 95% CI [-2.24 -0.72], p < 0.01; see Fig. 7b).
Fig. 7
a Forest plot of non-pharmacological interventions on depression. b Sensitivity analysis of non-pharmacological interventions on depression
留言 (0)