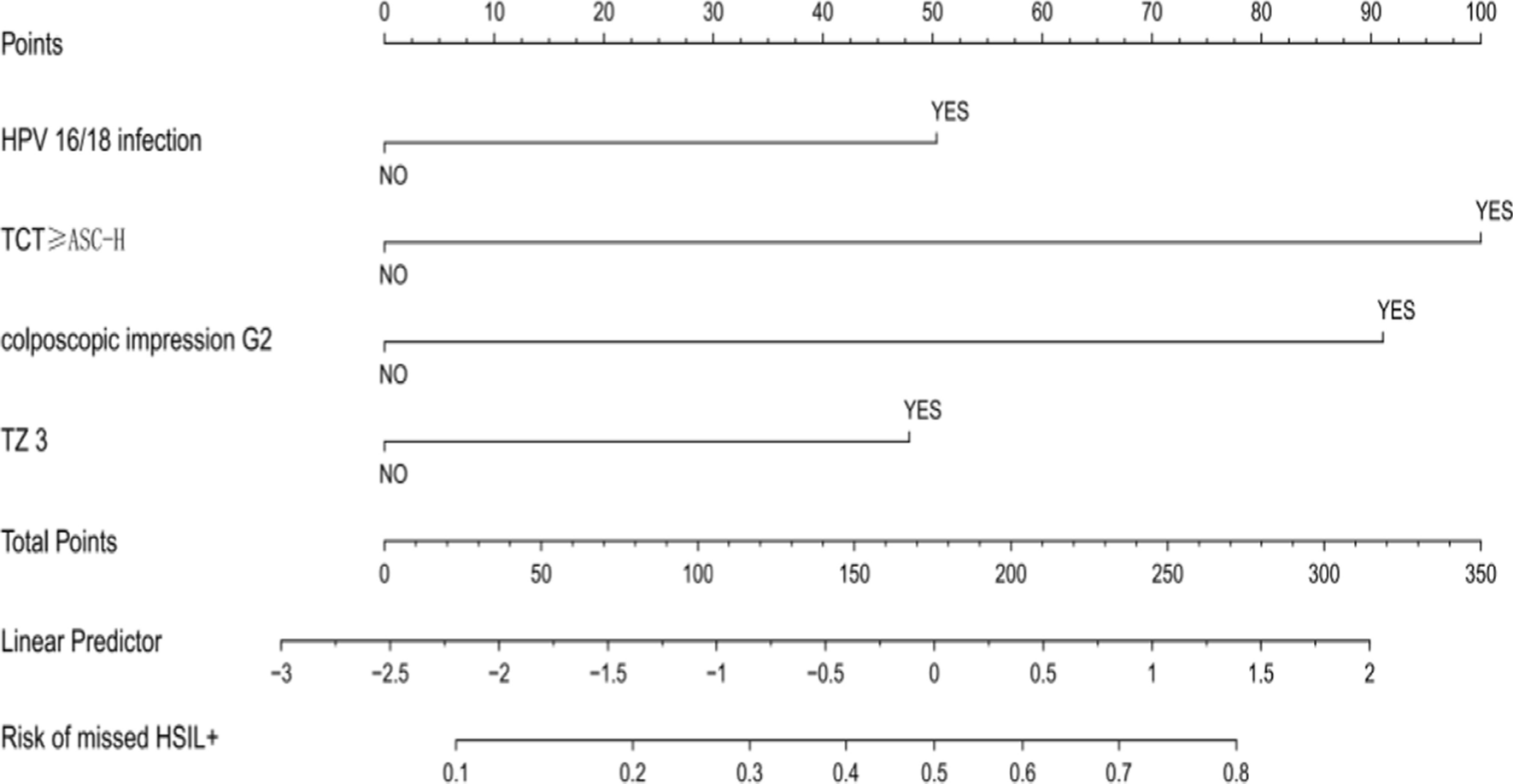
Low-grade squamous intraepithelial lesions (LSIL) arise as histological changes secondary to HPV infection, with approximately 80% of LSIL cases attributed to high-risk HPV (HR-HPV) infections [6]. This is supported by our study, which reported an HR-HPV infection rate of 88.1%. The complexity and transient nature of HPV infections make the management of LSIL challenging, often leading to missed diagnoses and overtreatment. Overtreatment can result in complications such as bleeding and stenosis, which may impede subsequent follow-ups [7]. Conversely, missed diagnoses increase the risk of progressing to cervical cancer [4, 5]. Consequently, clinical follow-up observation is the recommended management approach for LSIL, provided more severe lesions are excluded. In clinical practice, accurately identifying patients at risk of missed HSIL+ remains problematic. This challenge has led to the adoption of “risk stratification” as a strategy to standardize the management of LSIL [8]. Literature suggests that the rate of missed HSIL + diagnoses in patients with LSIL diagnosed by colposcopic biopsy ranges from 10 to 55% [4, 9]; our study aligns with these findings, presenting a missed diagnosis rate of 15.2%. For patients whose pathology was upgraded to HSIL after LEEP, we referred to the “Chinese Expert Consensus on the Management of High-grade Cervical intraepithelial Lesions” for management [2]. Factors associated with missed diagnoses in the literature include severe cytological abnormalities, extensive lesion range, transformation zone, immunosuppression, and gland involvement [10, 11]. Our findings confirm that HPV16/18 infection, TCT ≥ ASC-H, TZ3, and colposcopic impression G2 are independent risk factors for the missed diagnosis of HSIL+ . The nomogram model developed based on these factors demonstrated high predictive value.
Persistent HR-HPV infection, particularly with HPV16 and HPV18, is a well-recognized precursor to precancerous lesions and cervical cancer. In our cohort, 88.1% were infected with HR-HPV, 27.5% had HPV16/18 infections, and 31.9% had multiple HR-HPV infections, highlighting the significant role of HR-HPV in the etiology of cervical precancerous lesions. Studies have repeatedly shown that HPV16/18 infections significantly elevate the risk of developing HSIL+, with HPV16/18 positive women, even those with negative cytology, more likely to develop CIN2+ compared to those infected with other HR-HPV types [12]. Our analysis found that the rate of missed HSIL+ diagnoses was notably higher in women positive for HPV16/18 (25.2%) compared to those who were not (11.5%). Moreover, HPV16, known for its higher integration frequency with human genes, poses the greatest risk among HR-HPVs, making it the most prevalent type in HSIL+ cases [13]. A meta-analysis found that HPV16 accounts for 34–52% of all high-grade cervical lesions [14, 15], and a prospective cohort study indicated that women with HPV16 are significantly more likely to develop CIN2+ compared to those without HPV16 [16]. Given these data, HPV16/18 infections, particularly HPV16, emerge as crucial predictive markers for missed HSIL+ diagnoses in patients with LSIL, underscoring the importance of targeted HPV screening in this group.
Studies such as the Kaiser Permanente Northern California Medical Care Plan (KPNC) have highlighted the importance of prior cytology screening results in stratifying the risk of CIN3+ in women diagnosed with normal or ≤ CIN1 lesions by colposcopic biopsy [17]. For instance, women diagnosed with CIN1 and concurrent cytology of LSIL or HPV-positive ASCUS exhibited a 5-year risk of developing CIN3+ of 3.8%, whereas this risk escalated to 15% for those with CIN1 and cytology of HSIL [17]. These findings emphasize the significant role of cytology screening results in the stratified management of LSIL, an approach also endorsed by the Chinese expert consensus [1]. In our study, the missed diagnosis rates of HSIL+ corresponding to cytology of ASCUS, LSIL, ASC-H, and HSIL were 11.9%, 15.5%, 70.8%, and 60%, respectively. Notably, as cytological abnormalities increased, so did the rates of missed diagnoses. For patients with cytological findings of HSIL and ASC-H on a background of histologic LSIL, the 1-year risks of progressing to CIN3+ were 3.9% and 1.4%, respectively [18]. Furthermore, KPNC's findings suggest that women with cytologic ASC-H are at a risk level closer to HSIL than to LSIL [17], indicating that management protocols for cytology ASC-H should align more closely with those for cytology HSIL.In our cohort, the rate of missed diagnoses of HSIL+ was significantly higher in patients with TCT ≥ high-level lesion (66.7% vs. 10.9%). Moreover, patients with TCT ≥ ASC-H were found to have a 4.147-fold increased risk of a missed diagnosis of HSIL+. These insights underscore the necessity to enhance the stratified management of previous cytological results in patients with LSIL to mitigate the potential risk of occult HSIL+. Therefore, a more aggressive management approach is warranted for patients with cytologic findings of ASC-H/HSIL.
Transformation zones (TZs) are critical anatomical sites where precancerous lesions and invasive carcinomas typically develop. However, TZ visibility can vary, particularly in postmenopausal women, where age-related changes often retract the TZ into the cervical canal and, combined with epithelial atrophy, can complicate biopsy collection, thereby increasing the risk of missed diagnosis of cervical intraepithelial neoplasia (CIN). Studies have reported varying accuracy rates for detecting CIN2+ across different TZ types: 92.2% for TZ1, 90.5% for TZ2, and 76.5% for TZ3 [19]. In cases with low-grade colposcopic impressions and TZ3, missed diagnosis rates for CIN2 and CIN3 are notably higher (52.6% and 31.6%, respectively) compared to TZ1/2 (27.5% and 18.8%) [20]. In our study, the rates of missed HSIL+ diagnoses were 8.5% for TZ1, 16.9% for TZ2, and 25% for TZ3, indicating a significant increase in missed diagnoses in patients with TZ3. Caution is therefore necessary when interpreting nonrepresentative biopsies from women with TZ3, and employing endocervical curettage (ECC) may enhance HSIL+ detection in these cases [21].
Colposcopy plays a vital role in cervical cancer screening by localizing lesions in the lower genital tract, guiding biopsies, and informing management strategies. It also assists in the follow-up after treatment. Historical data indicate that the agreement between histopathological diagnosis and colposcopic diagnosis ranges from 52 to 99% [22]. In this study, among 382 patients with a low-grade colposcopic impression, the concordance between cervical biopsy diagnosis and colposcopy was 75.6%, while the agreement between postoperative diagnosis and colposcopy diagnosis was 89%, aligning with prior findings. Given that colposcopy's effectiveness can be influenced by the examiner's experience and is somewhat subjective, approximately 10% of HSIL cases may still be overlooked, even when biopsy pathology under colposcopy indicates LSIL [9]. For patients referred for colposcopy with LSIL, 9.9% were found to have CIN2+ under a low-grade colposcopic impression [23]. A meta-analysis revealed that the overall risk of CIN2+ for women with a low-grade colposcopic impression ranges widely from 11 to 69%, depending on the screening context [24]. Furthermore, 30% of women with grade 2 colposcopy findings have HSIL/CIN3, irrespective of screening test results [20]. In our study, 11% of women with a low-grade colposcopic impression and 57.1% with a high-grade impression were diagnosed with HSIL+. These findings underscore the importance of standardized, safe, and accurate colposcopy, with quality control being essential to maximize colposcopy’s value in preventing and treating cervical cancer.
Machine learning is an important branch of artificial intelligence. In medicine, machine learning technology is changing the way we diagnose, treat, and manage disease. Machine learning can help us extract valuable information from massive medical data, and build predictive models based on the processing data to improve the diagnosis accuracy of diseases, predict the development trend of diseases and optimize treatment plans. Machine learning has brought tremendous insight and predictive power to the medical industry and is increasingly being used in the medical field. For example, Our center has done some research on machine learning and HSIL. Zeng constructed a logistic regression model based on risk factors to predict the risk coefficient of residual lesions after cervical conization in patients with HSIL,The AUC calculated by logistic regression model was 0.78 [25]. This model is being further validated and is expected to be used in clinical practice. Zhang conducted a retrospective analysis of 3343 patients who underwent CKC for HSIL, and then applied seven machine learning methods to construct a positive margin risk prediction model, logistic regression model has the best predictive performance,with an accuracy of 74.7%, sensitivity of 76.7%, specifcity of 74.4%, and AUC of 0.826 [26]. Machine learning can often build some better prediction models with improved accuracy and sensitivity due to its diversity and uniqueness of methods and relatively advanced algorithms.
Through univariate and multivariate analyses of collected data, we identified independent risk factors for the missed diagnosis of HSIL+. Utilizing these factors, we constructed predictive models for HSIL+ using machine learning methods. Machine learning, with its diverse methodologies and advanced algorithms, often surpasses traditional logistic regression models in accuracy and sensitivity. Our comparative analysis across the training and validation set revealed that the Decision Tree model demonstrated the most effective predictive performance.
The predictive models we developed offer two significant advantages: simplicity of operation and cost-effectiveness. The model can be programmed and stored on a computer. Clinicians simply input the patient's data for specific indicators, and the program automatically calculates the risk of missed diagnosis of HSIL+. This aids in the early identification of patients at high risk of missed diagnosis of HSIL+. Additionally, the indicators required by our model are straightforward, derived from routine medical inquiries and examinations, eliminating the need for costly tests, invasive procedures, or any invasion of patient privacy.For patients identified as high-risk through preoperative examinations, clinicians should diligently assess the risk of HSIL+ and consider selective diagnostic coning if necessary. Moreover, such patients should be closely monitored post-surgery to minimize the chances of residual disease and recurrence.
However, our study is not without limitations. Firstly, the sample size is relatively small, characterizing this as a small-sample study. Secondly, instead of using a prospective cohort design and following up with patients predicted to be at high risk, we conducted a retrospective study, which may introduce selection bias. Additionally, the training and validation set data were sourced from the same hospital, which could limit the applicability of our model in other settings with different surgical techniques and protocols.
In conclusion, our study identifies several independent risk factors for the missed diagnosis of HSIL+ in patients with LSIL diagnosed by colposcopic biopsy, including HPV16/18 infection, TCT ≥ ASC-H, TZ3, and colposcopic impression G2. The clinical prediction model developed in this study demonstrates robust consistency and practical value, offering significant guidance for clinicians in reducing the risks of missed diagnosis of HSIL+ and the overtreatment of LSIL.



留言 (0)