
記住我


All patients enrolled in the study were followed, the median follow-up time was 61.0 months (3.0–152.0 months). The median age of the 941 patients was 56.0 years (45.0–65.0 years), and 489 (52.0%) patients were male. HBsAg + patients were significantly younger at diagnosis (median age, 51.6 vs. 55.0), had an advanced stage (proportion of patients with stage III-IV disease: 60.9% vs. 47.5%, P = 0.021), and had more GCB subtypes (37.0% vs. 26.8%, P = 0.041), B symptoms (39.9% vs. 28.5%, P = 0.007), spleen involvement (23.9% vs. 7.0%, P < 0.001), elevated β2-MG (60.1% vs. 55.0%, P = 0.008) and AST levels (21.7% vs. 10.2%, P < 0.001) (Table 1).
Table 1 Clinical characteristics of HBsAg positive and HBsAg negative diffuse large B-cell lymphoma patientsHBV-RA total of 138 patients with HBsAg + DLBCL and 473 patients with HBsAg−/HBcAb + DLBCL were included in the study, and a total of 26 (4.3%, 26/611) patients developed HBV-R. The median time from first chemotherapy to HBV-R was 12 months. Compared with HBsAg−/HBcAb + DLBCL patients, HBsAg + DLBCL patients had a greater rate of HBV-R (15.2% vs. 1.1%, P < 0.001). The use of CD20 monoclonal antibodies did not increase the HBV reactivation rate in HBsAg + DLBCL patients (16.1% vs. 7.1%, P = 0.621) or HBsAg−/HBcAb + patients (1.1% vs. 0%, P = 1.000). Anti-HBV prophylaxis did not decrease the HBV-R rate in HBsAg + /HBV DNA- patients (21.6% vs. 26.7%, P = 0.949) or HBsAg−/HbcAb + patients (1.1% vs. 1.0%, P = 1.000), but HBsAg + /HBV DNA- patients had more HBV-R than HBsAg−/HbcAb + patients despite receiving anti-HBV prophylaxis (21.6% vs. 1.1%, P < 0.001). Nine patients in the study developed HBV-R-related hepatitis, and all of these patients were treated with R-CHOP/R-CHOP-like regimens. The incidence of HBV-R-related hepatitis was greater in patients with HBsAg + DLBCL than in those with HBsAg−/HBcAb + DLBCL (5.1% vs. 0.4%, P < 0.001).
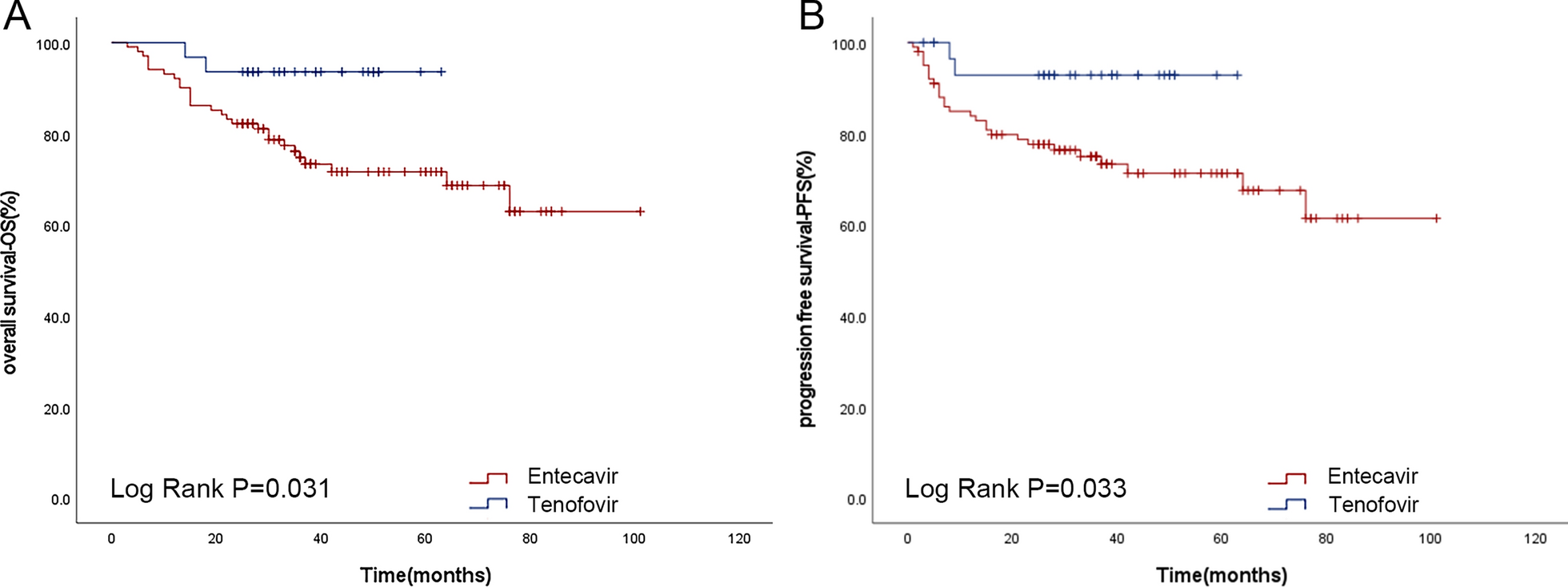
In this study, 292 patients received prophylactic anti-HBV treatments. A total of 18 (6.2%, 18/292) patients developed HBV-R, of which 8 (8/114, 7.0%) patients were treated with Lamivudine, 7 (7/129, 5.4%) patients were treated with Entecavir, and 1 (1/42, 2.4%) patient was treated with Tenofovir. HBV-R developed in 1 of 6 patients who had received multi-drug anti-HBV therapy. Only 1 patient was treated with Adefovir, and that patient developed HBV- R. There is no significant difference in HBV-R when lamivudine, entecavir, or tenofovir was used for anti-HBV therapy (P = 0.605). Additional analyses revealed tenofovir improved patients' OS and PFS more than did entecavir (χ2 = 4.644, P = 0.031; χ2 = 4.554, P = 0.033) (Fig. 1).
Fig. 1
Kaplan‒Meier analysis of the OS (A) and PFS (B) in patients with primary DLBCL treated with prophylactic anti-HBV therapy with entecavir and tenofovir after June 17, 2014.OS: overall survival; PFS: progression-free survival; DLBCL: diffuse large B-cell lymphoma; HBV: hepatitis B virus
Efficacy and survival outcomesEfficacyA total of 637 patients (67.7%, 637/941) achieved CR, and 203 patients (21.6%, 203/941) achieved PR; the overall remission rate (ORR) was 89.3%. 29 patients (50.9%, 29/57) achieved CR, 15 patients (26.3%, 15/57) achieved PR among patients treated with CHOP/CHOP-like regimens, with an ORR of 77.2%; 608 patients (68.8%, 608/884) achieved CR, and 188 patients (21.3%, 188/884) achieved PR among patients treated with R-CHOP/R-CHOP-like regimens, with an ORR of 90.0%. The ORR was similar in HBsAg + DLBCL, HBsAg−/HBcAb + DLBCL, and HBsAg-/HBcAb-DLBCL patients (87.0% vs. 90.1% vs. 89.1%, P = 0.579).
Treatment of HBsAg + DLBCL and HBsAg−/HBcAb-DLBCL patients with R-CHOP/R-CHOP-like regimens was more effective than treatment with CHOP/CHOP-like regimens, but there was no statistically significant difference in efficacy between these two chemotherapy regimens in HBsAg−/HBcAb + DLBCL patients (Supplementary Table S1). Relapse after treatment was more common in HBsAg + DLBCL patients than in HBsAg−/HBcAb + DLBCL and HBsAg−/HBcAb-DLBCL patients (10.9% vs. 5.3% vs. 5.8%, P = 0.052).
Survival outcomesAt the end of follow-up, 243 patients (25.8%, 243/941) in this cohort had died—38 patients (27.5%, 38/138) in the HBsAg + group, 124 patients (26.2%, 124/473) in the HBsAg−/HBcAb + group, and 81 patients (25.4%, 81/330) in the HBsAg−/HBcAb− group—and the median OS and PFS of all patients were not reached.
The 5-year OS rates for DLBCL patients in the HBsAg + , HBsAg−/HBcAb + , and HBsAg-/HBcAb- groups were 76.0% versus 74.4% versus 77.4%, respectively; the median OS was 121 months in the HBsAg-/HBcAb + group and was not reached in either the HBsAg + or HBsAg−/HBcAb− group (χ2 = 0.139, P = 0.933); the 5-year PFS rates in the three groups were 71.3% versus 73.9% versus 76.3%, respectively; and the median PFS was not reached in any of the three groups (χ2 = 0.787, p = 0.675). Both the median OS and PFS were greater in the R-CHOP/R-CHOP-like group than in the CHOP/CHOP-like group (not reached vs. 68 months, χ2 = 21.686, P < 0.001; not reached vs.48 months, χ2 = 26.776, P < 0.001) (Fig. 2).
Fig. 2
Kaplan‒Meier analysis of the OS and PFS in patients with different HBV serologic statuses and different chemotherapy regimens. OS (A) and PFS (B) in patients with different HBV serologic statuses. OS (C) and PFS (D) in patients treated with different chemotherapy regimens. OS: overall survival; PFS: progression-free survival; HBV: hepatitis B virus
Among the 138 HBsAg + DLBCL patients, 14 (10.1%) patients received CHOP/CHOP-like regimens, and 124 (89.9%) patients received R-CHOP/R-CHOP-like regimens. The 3- and 5-year OS rates were 57.1% versus 81.9% and 49.0% versus 79.6%, respectively, in the two groups, and the R-CHOP/R-CHOP-like group had a better median OS than did the CHOP/CHOP-like group (not reached vs. 56 months, χ2 = 7.679, P = 0.006); the 3- and 5-year PFS rates were 48.7% versus 79.6% and 29.2% versus 76.8%, respectively, in the two groups, and the median PFS was also better in the R-CHOP/R-CHOP-like group (not reached vs. 33 months, χ2 = 9.042, P = 0.003).
There were 473 HbsAg−/HbcAb + DLBCL patients, 30 (6.3%) in the CHOP/CHOP-like group and 443 (93.7%) in the R-CHOP/R-CHOP-like group; the 3- and 5-year OS rates were 60.0% versus 82.6% and 56.7% versus 75.3% in the two groups, respectively; the 3- and 5-year PFS rates were 53.6% vs 79.7% and 49.1% vs 75.1% in the two groups, respectively; and both OS and PFS were better in the R-CHOP/R-CHOP-like group (median OS: 121 months vs. 83 months, χ2 = 7.146, P = 0.008; median PFS: not reached vs. 77 months, χ2 = 9.515, P = 0.002).
Among the 330 HbsAg-/HbcAb-DLBCL patients, 13 patients (3.9%) were in the CHOP/CHOP-like group, and 317 patients (96.1%) were in the R-CHOP/R-CHOP-like group; the 3-year and 5-year OS rates in the two groups were 46.2% versus 82.1% and 46.2% versus 78.7%, respectively; the 3-year and 5-year PFS rates were 46.2% versus 80.1% and 36.9% versus 76.8%, respectively; and the R-CHOP/R-CHOP-like group remained superior in terms of OS and PFS (median OS: not reached vs. 29 months, χ2 = 8.039, P = 0.005; median PFS: not reached vs. 24 months, χ2 = 8.317, P = 0.004) (Fig. 3).
Fig. 3
Kaplan‒Meier analysis of the OS and PFS of patients receiving different chemotherapy regimens. OS (A) and PFS (B) in HBsAg + DLBCL patients treated with CHOP/CHOP-like or R-CHOP/R-CHOP-like regimens; OS (C) and PFS (D) in HBsAg-/HBcAb + DLBCL patients treated with CHOP/CHOP-like or R-CHOP/R-CHOP-like regimens; OS (E) and PFS (F) in HBsAg-/HBcAb-DLBCL patients 28 treated with CHOP/CHOP-like or R-CHOP/R-CHOP-like regimens. OS: overall survival; PFS: progression-free survival; CHOP: cyclophosphamide, doxorubicin, vincristine, prednisone; R-CHOP: CHOP plus rituximab; HBsAg + : hepatitis B virus surface antigen positive; HBsAg-/HBcAb + : hepatitis B virus surface antigen negative/core antibody positive; HBsAg-/HBcAb-: hepatitis B virus surface antigen negative/core antibody negative; DLBCL: diffuse large B-cell lymphoma
After excluding 23 patients with missing information, we analyzed survival outcomes in 918 patients with different COO subtypes. In HBsAg + DLBCL patients, there was no significant difference between GCB and non-GCB subtypes in OS and PFS (χ2 = 0.101, P = 0.751; χ2 = 0.404, P = 0.525). GCB and non-GCB subtypes in HBsAg-/HBcAb + and HBsAg-/HBcAb- patients similarly did not show a significant difference (HBsAg−/ HBcAb + : OS: χ2 = 0.415, P = 0.520; PFS: χ2 = 0.454, P = 0.500; HBsAg-/HBcAb-: OS: χ2 = 1.260, p = 0.262; PFS: χ2 = 1.093, p = 0.296) (Supplementary Fig. 1).
Prognostic factorsPrognostic factors in HBsAg + DLBCL patientsAccording to the univariate analysis, female sex, age > 60 years, elevated LDH and ECOG score ≥ 2 were risk factors for OS; ECOG score ≥ 2, elevated LDH and IPI score > 3 were risk factors for PFS in HBsAg + DLBCL patients. Multivariate analysis revealed that female sex, age > 60 years, elevated LDH, rituximab used and anti-HBV prophylaxis were found to be independent prognostic factors affecting OS, and the above five factors with an ECOG score ≥ 2 were prognostic factors affecting PFS. The use of rituximab and anti-HBV prophylaxis were protective factors for OS and PFS in HBsAg + DLBCL patients (Table 2).
Table 2 Risk factors for OS and PFS in HBsAg + DLBCL patientsPrognostic factors in HBsAg-/HBcAb + DLBCL patientsUnivariate analysis revealed that age > 60 years, advanced stage disease (stage III or IV), liver involvement, extranodal involvement ≥ 2, elevated LDH, and IPI ≥ 3 were associated with inferior OS and PFS in HBsAg-/HBcAb + DLBCL patients. Multivariate analysis revealed that age, rituximab used, and disease stage were prognostic factors affecting OS and PFS in patients, and the administration of rituximab improved the prognosis of HBsAg−/HBcAb + DLBCL patients (Table 3).
Table 3 Risk factors for OS and PFS in HBsAg-/HBcAb + DLBCL patientsPrognostic factors in HBsAg-/HBcAb-DLBCL patientsAccording to the univariate analysis, advanced disease stage (stage III or IV), elevated LDH, an IPI ≥ 3 and rituximab were prognostic factors for OS in patients with HBsAg-/HBcAb-DLBCL, and the above four factors plus an ECOG score ≥ 2 were prognostic factors for PFS. Multivariate analysis revealed that prognostic factors for OS in HBsAg-/HBcAb-DLBCL patients included advanced disease stage, elevated LDH, and GCB type cell origin. Advanced disease stage, elevated LDH, GCB type cell origin and rituximab used affected PFS in HBsAg-/HBcAb-DLBCL patients (Supplementary Table S2).
留言 (0)