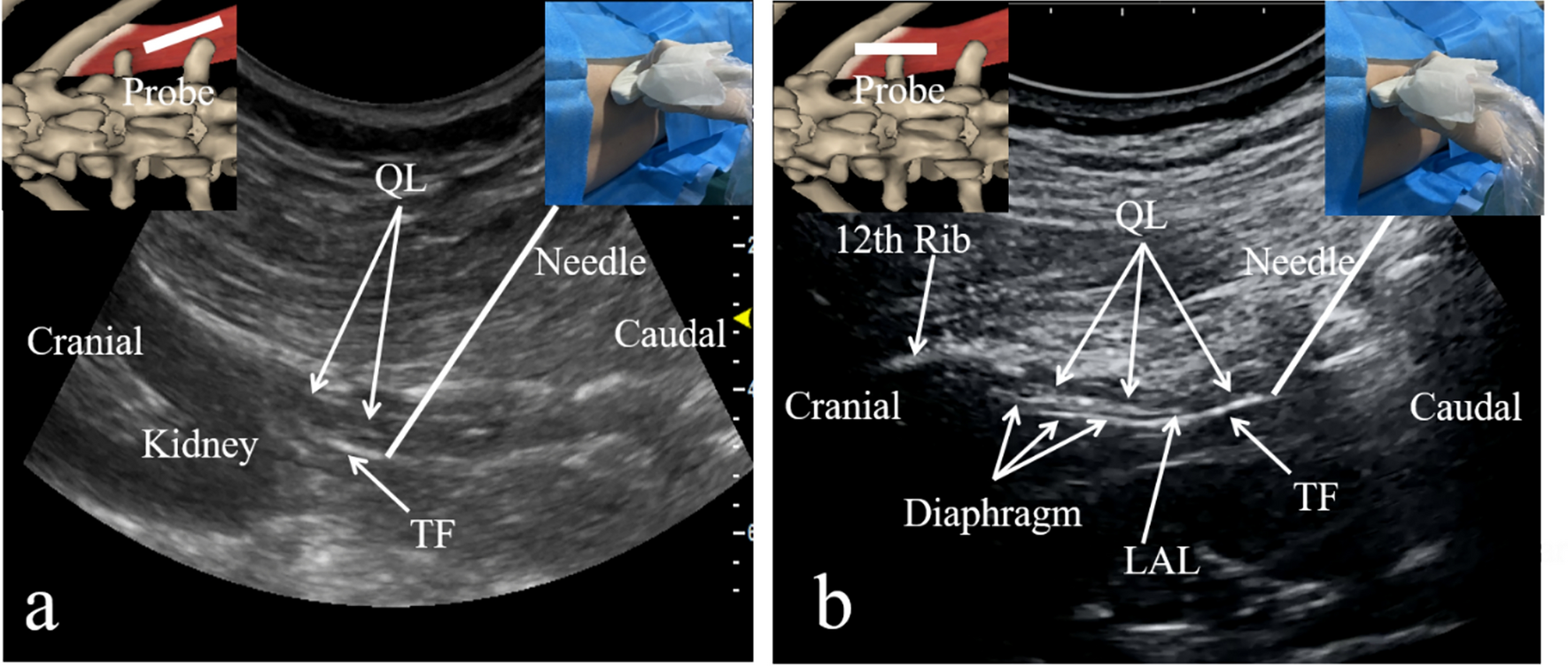
Herein, we describe a new ultrasound-guided ONB approach performed in a case series of six patients undergoing TURBT, with a cadaveric investigation. We confirmed that the needle tip can be placed in the distal end of the obturator canal under ultrasound guidance with patients in the lithotomy position.
Anagnostopoulou et al. [1] reported that bifurcation of the obturator nerve into the anterior and posterior branches variably occurs within the pelvic cavity, obturator canal, and medial thigh in 23.22%, 51.78%, and 25% of the specimens, respectively. In some specimens, the posterior branch passes through the obturator externus muscle immediately after emerging from the obturator canal, which means that it does not exist between the obturator externus and pectineus muscles [1, 8]. Moreover, the articular branches to the hip joint arise from the common obturator nerve or its divisions at various levels [1]. Therefore, the articular branches do not always lie between the obturator externus and pectineus muscles. Consequently, constraining local anesthetic infiltration only to the intermuscular space, the target of previously reported ultrasound-guided proximal ONB approaches, does not guarantee blockade of the posterior and hip articular branches of the obturator nerve. When the local anesthetic fills the obturator canal, the obturator nerve, including its anterior and posterior divisions and the hip articular branches, are blocked given that all these nerve fibers unexceptionally run through the obturator canal [1, 11]. When 10 ml of the solution was injected at the distal end of the obturator canal using our approach, we noted that only a small amount of the local anesthetic solution overflowed from the obturator canal, as seen in Supplementary Video 1. This implied that most of the injected local anesthetic entered the obturator canal, as predicted and confirmed in our cadaveric examination.
A potential advantage of our current approach over our previous proximal ONB technique [5] would be the feasibility of directly delivering local anesthetic into the obturator canal.
Therefore, our current approach to filling the obturator canal with local anesthetic may reduce the required local anesthetic volume compared to previously reported proximal approaches. Nevertheless, a dose-finding study is needed to confirm this postulation. To ensure a wide safety margin, we determined the use of 10 ml of local anesthetic, as used in previous research regarding the conventional proximal ONB approach [8]. Concerning possible disadvantages, the angle between the needle trajectory and ultrasound beams is smaller with our current approach than with our previous approach, leading to less needle visibility under ultrasound guidance.
Our study has some limitations. Our findings are based on only six cases and one cadaveric examination. Moreover, we did not specifically assess the effects of the ONB, although this study aimed to demonstrate the feasibility of seeing the obturator canal, placing the needle tip at the external orifice of the canal under ultrasound guidance, and performing an ONB. Furthermore, we did not employ nerve stimulation to locate the obturator nerve. Since all nerve fibers arising from the obturator nerve run through the obturator canal [1, 11], injecting a local anesthetic into the obturator canal should produce the ONB without the need for locating the nerve. However, for safety reasons, we should have combined nerve stimulation with our new ultrasound-guided ONB technique, because the movement of the adductor muscles must be controlled during TURBT. Nerve stimulation can also be helpful to avoid direct obturator nerve injury during needle advancement.
In summary, this case series, combined with a cadaver examination, provides a good foundation for future studies to confirm the usefulness of our ultrasound-guided obturator canal approach for ONB.


留言 (0)