The present study aimed to determine and compare the predictive power of novel versus conventional anthropometric parameters for identifying metabolic syndrome in the Bandare-Kong population in the south of Iran. In clinical practice, anthropometric indices such as AVI, WHtR, and WC could be useful for identifying individuals at risk of metabolic syndrome. These indices are non-invasive, easily measurable, and low-cost options and can be easily incorporated into routine screenings to help identify at-risk patients, particularly in resource-limited healthcare settings. We evaluated these indexes in overweight/obese and non-overweight/obese subjects of both genders. According to our findings, the overall prevalence of Mets was 29.8% (male:12.8% and female:17.0%), which is lower than previous studies in other parts of Iran and some other countries [18,19,20].
We found the weakest correlation between ABSI and metabolic components, which is consistent with previous studies [21,22,23,24]. However, most other anthropometric measures exhibited a significant correlation with metabolic variables. Further, a non-MetS parameter, LDL-C, showed the lowest correlation with anthropometric indices in females. The results demonstrated that most obesity indices were significantly associated with metabolic syndrome, especially in participants with BMI < 25 (non-overweight/obese), except for ABSI and slightly WWI. This is in accordance with a recent study by Lihong et al. in China [25].
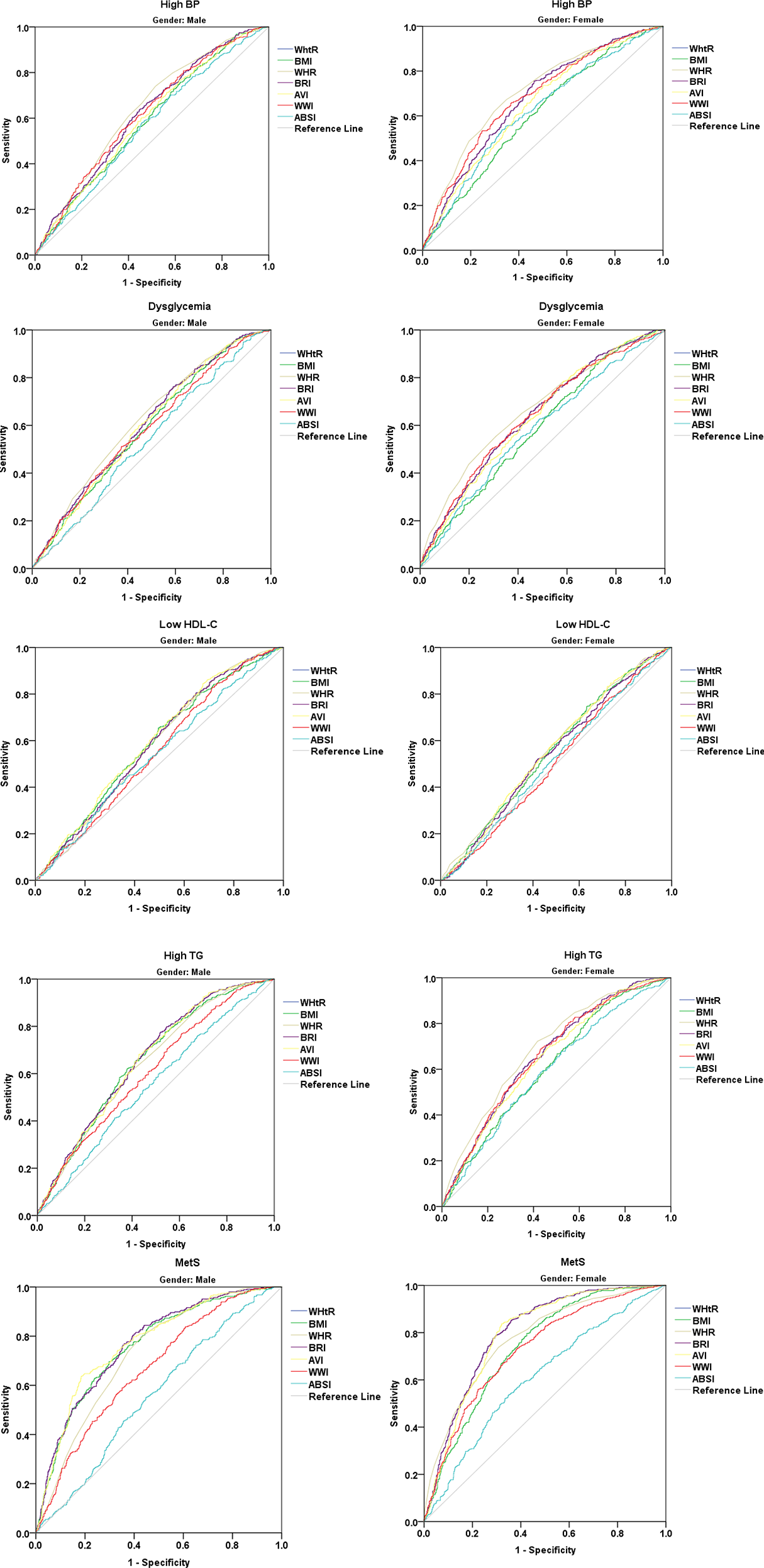
In both genders, binary logistic analyses revealed significant relationships between anthropometric indices and MetS, especially for WHtR and BRI. Even though some published studies have shown an association between ABSI and metabolic syndrome, we found only a weak correlation with MetS recognition [26, 27]. Further assessment according to BMI showed that AVI had a robust relationship with MetS in subjects with BMI < 25, but the extent of this connection, though still significant, decreased in subjects with BMI > 25. The estimated pooled AUC by gender for WHtR, BRI, and AVI to predict MetS were more than others. However, these amounts were the least for WWI and ABSI. This aligns with the findings of Behboudi et al., who similarly reported that ABSI lacked efficacy as a predictor for MetS [28]. Consistently, other studies in China indicated that ABSI failed to predict MetS in both genders [29, 30]. Khan et al. also observed that WHtR and AVI had significantly higher mean AUC values compared to other metrics [31]. Further stratification based on BMI revealed slightly different results. WHR and AVI emerged as having the highest AUC, while WHtR and BRI demonstrated a similar AUC, suggesting a comparatively better ability to determine MetS. Notably, among non-overweight subjects, WHR marginally outperformed AVI as the most effective identifier of MetS, while in overweight/obese individuals, AVI showed a slightly superior ability compared to WHR. Wu et al.‘s investigation in non-overweight/obese adults corroborated this by highlighting AVI’s superior capability to determine MetS [25]. This study emphasized the diverse predictive power of anthropometric indices for different components of MetS. Consequently, choosing the most suitable marker for clinical use would depend on the specific metabolic elements requiring assessment. For instance, WHR exhibited the highest AUC for high blood pressure in both genders, whereas BMI and ABSI showed the lowest values. Conversely, AVI and BMI demonstrated the largest AUC for low HDL in men, whereas in women, it was WHR and AVI. Guo et al. concluded that while all obesity indices showed a similar capacity to predict MetS overall, there were sex-based differences. BMI demonstrated the largest AUC in men, while WHtR and BRI exhibited this in women [32].
A pairwise comparison of ROC curves for MetS identification power by gender revealed no significant differences between WHtR, BRI, and AVI in males. However, there were significant disparities between the other measures. In females, WHtR, WHR, BRI, and AVI all showed statistically similar prediction abilities. In participants with BMI < 25, there were no significant differences between WHtR and BRI in the ability to predict MetS, as well as between WWI and ABSI. According to the comparison results for individuals with BMI > 25, there were no statistically significant differences between WHR and AVI, nor were there significant differences between WHtR, WHR, and BRI. The lack of significant differences in these anthropometric indices’ ability to detect MetS may reflect the strong correlations between these indices, as they share similar underlying variables, such as waist circumference, as well as their shared ability to capture similar aspects of central obesity and overall body fat distribution. This similarity limits their ability to provide distinct predictive power.
The proposed optimal cut-off value for each anthropometric index to determine MetS showed that WHR had the highest sensitivity and AVI had the highest specificity in males. However, WHtR and BRI displayed the highest sensitivity, and WHR displayed the highest specificity among females. This suggests that in clinical practice, we should use gender-specific parameters. The results of this study indicated that although most indicators were more sensitive in females, they were less sensitive in males. We found that the optimal WHtR cut-off value (0.52) for identifying MetS in a Chinese study was similar to our results [33]. In a separate study [34], Baveicy et al. found similar cut-off values for men and women (4.75 and 6.17, respectively). In subjects with BMI < 25, WHR and WWI had the highest optimal cut-off values’ sensitivity and specificity, respectively. Nevertheless, for people with BMI > 25, AVI and WWI had the highest optimal cut-off value sensitivity and specificity, respectively.
There are certain limitations and strengths to the current study that should be acknowledged. As this is a cross-sectional study, a prospective cohort study could be used to verify the conclusions. Since this is a cross-sectional study, it only allows for the evaluation of associations between anthropometric indices and MetS and cannot establish a cause-effect relationship or assess the risk of developing MetS over time. Future prospective studies are needed to establish causal relationships.
In addition, the participants were from the same ethnic group and shared a similar lifestyle and culture. As a result, future studies should be conducted in multiethnic populations to ensure that the results are applicable to a wider population. This study possesses critical strength in that it stratifies anthropometric indices in obese and non-obese individuals, as well as takes gender analysis into account. Moreover, we analyzed cut-points for each indicator separately for men and women and obese and non-obese populations.


留言 (0)