This study assessed incidence of T2DM among Ghanaian cohorts living with HIV initiated on a DTG based antiretroviral therapy. The incidence proportion and rate of T2DM was 11.8% and 98.1 cases per 1000 PY respectively. Male participants and those aged ≥ 50 years had a higher risk of developing T2DM compared to being female and aged < 50 years respectively. Being male, having abnormal waist-hip ratio and abnormal total serum cholesterol were significant determinants of T2DM.
Our study revealed a T2DM incidence proportion of 11.8% with a median time to development of 24 weeks after initiation onto DTG. This is similar to findings from O’Halloran et al. which reported use of INSTI to be associated with 31% increased risk of new-onset hyperglycemia within 24 weeks of follow up [25]. In another study in Uganda, patients on DTG based regimen had seven times greater odds of developing diabetes compared to DTG naïve patients [14]. Similar findings of T2DM and its association with DTG have been reported in some studies in sub-Saharan Africa [16, 26, 27]. The first 24 weeks post DTG initiation for hyperglycemia is important in monitoring of patients for early interventions to avert progression to T2DM. Though the underlying mechanism for DTG associated hyperglycemia in our patients is unknown, their glycemic status was established at baseline as having normal fasting glucose levels. Thus, DTG may likely have a role to play and further studies are needed in this area to investigate genetic polymorphisms and role of DTG in influencing glucose metabolism.
However, contrary to our study findings, a systematic review of ten articles with a total of 62,400 participants on INSTI and risk of development of T2DM with follow up periods varying from one year to eighteen years, reported there was no statistically significant difference in T2DM among PLHIV on INSTIs compared to those treated with protease-inhibitors (PI) [17]. The review also reported a lower incidence of T2DM in PLHIV on INSTIs compared to those using non-nucleoside reverse transcriptase inhibitors (NNRTIs) [17]. Another systematic review of thirteen articles by Mulindwa et al. with a patient population of 72,404, reported a lower risk of T2DM compared with NNRTIs although not statistically significant [28]. The risk was however similar to those on protease inhibitor-based therapy but increased in the African population [28]. The difference in finding may be due to different geographical context as only 3 out of the 23 articles were from Africa (Uganda, Cameroon, and South Africa). Also, the study designs employed in the articles from Cameroon and South Africa were both randomized control trials whilst that from Uganda was a case-control [28]. Our study was a prospective one in a real-world setting, and this could account for the current findings being reported. The difference in geographical setting and genotypic characteristics of PLHIV will need further studies to evaluate if these differences play a major role in risk of developing T2DM. However, the increased incidence proportion of T2DM among our study participants corroborates with increased risk of T2DM in African population reported by Mulindwa et al. [28].
In this study, the incidence proportion and rate of T2DM was higher (12.6% and 101.4 per 1000PY) among ART experienced compared to 6.5% and 68 per 1000PY among ART-naïve patients. The association between being ART experienced and risk of developing T2DM was however, not statistically significant. This is in contrast to several studies including the Multicenter AIDS Cohort Study, VIKING-3 study, SPRING-2 and SINGLE studies [14, 29,30,31,32,33] which found that patients who were ART experienced have an increased risk of developing T2DM. This could be due to the fact that patients who have been on ART for long were probably exposed to agents from the first-generation ART, which are known to have notable metabolic toxicities resulting in insulin resistance [34]. Another study in South Africa reported increase in odds by more than three-folds of developing T2DM in ART experienced patients compared to ART naïve [18]. Another cohort study among 243 ART-naïve patients all receiving DTG from Uganda also reported a low incidence (4 cases per 1000 PY (1/243)) of T2DM although their sample size was small [14]. This buttress reports of increased risk of T2DM in ART experienced compared to ART-naïve patients. Therefore, it is important for clinicians to assess ART-experienced patients for risk factors for T2DM and keenly monitor them regularly for hyperglycemia as part of the clinical package when transitioned to DTG.
Being male was significantly associated with T2DM in our study and had about 3 times increased risk of developing T2DM compared to females. This was similar to reports by Lamorde et al. in Uganda where 81.3% of patients with DTG-associated hyperglycemia were males [35]. However, this was subject to confounding as majority of the study participants were males. Contrary to these findings, another study in Uganda did not find any association between males on DTG and risk of T2DM [16].
Our study also showed that patients aged ≥ 50 years had a 64% increased risk of developing T2DM. This is similar to findings from a Ugandan study where patients on DTG based regimen aged ≥ 56 years had twelve times the odds of developing hyperglycemia compared to those aged 18–35. Older age is one of the traditional risk factors for T2DM. Age-related impairment of pancreatic islet function and increasing insulin resistance collectively increase the risk of T2DM among older patients [36]. Older patients at high risk of T2DM should be considered for alternate regimen rather than DTG-based regimen to reduce risk of T2DM or be subject to more rigorous monitoring for early detection and institution of interventions.
In our study, the incidence of T2DM was higher among patients with elevated total cholesterol compared to those with normal levels of total cholesterol. Elevated total serum cholesterol was associated with 61% increased risk of developing T2DM in this study. Studies evaluating DTG use and lipids have reported no significant changes seen in the lipids including total cholesterol [37, 38]. Patients on efavirenz who switched to DTG were found to have reductions in lipids [38]. Though published reports indicate DTG may be of great benefit to patients with a high risk of cardiovascular disease due to lipid reduction, this needs careful interpretation as patients with elevated lipids are at risk of hyperglycemia.
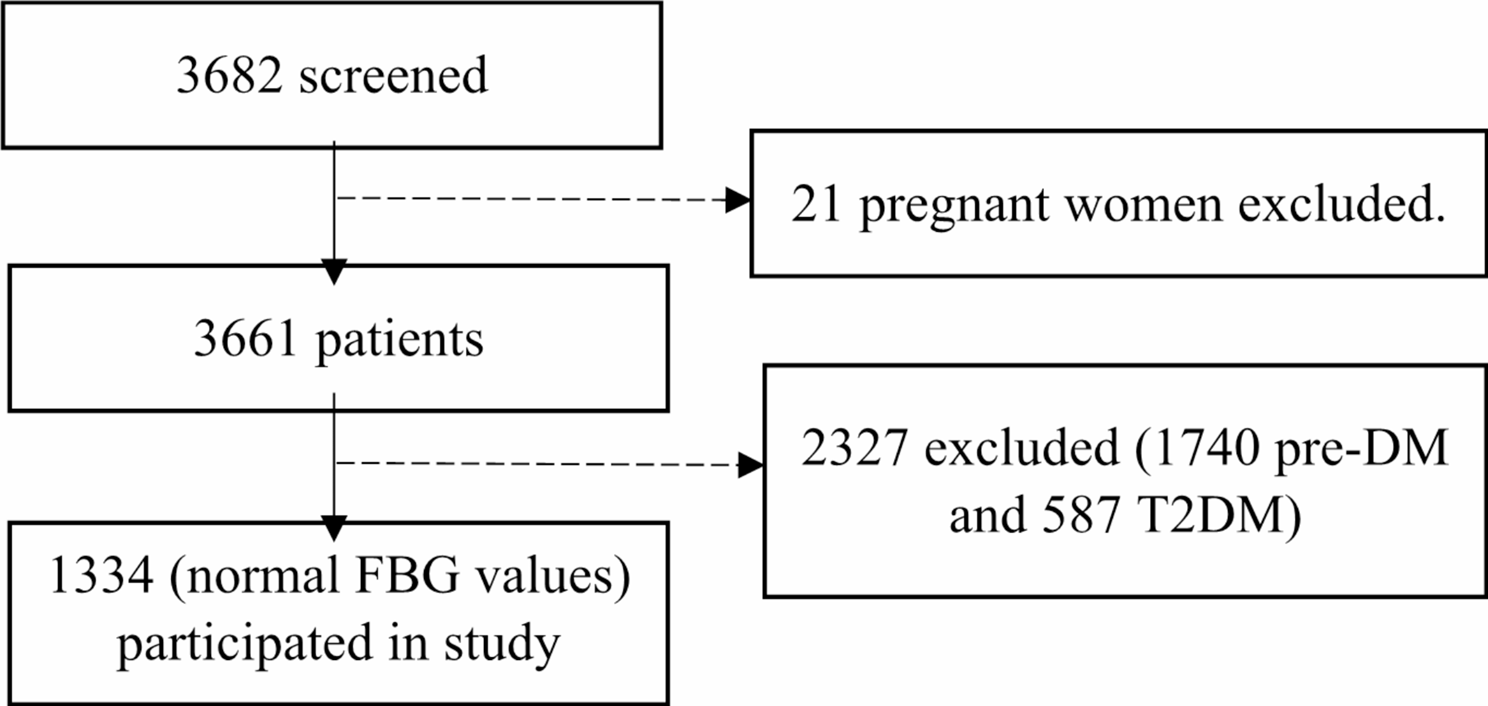
Our study showed that over 60% of our study participants had high levels of pre-DM and T2DM during the screening phase which had not been earlier diagnosed. Though HIV and ART are contributing factors to NCDs among PLHIV [6, 7, 9, 10], the reasons for these high levels of pre-DM and T2DM are unclear. These participants were excluded from the study however this raises the issue of further research into the aetiopathogenesis of DM and especially in PLHIV. Genotypic and phenotypic factors may play a significant role in the development of hyperglycemia and even idiosyncratic drug reactions may be considered. More rigorous mechanistic studies need to be conducted among PLHIV to provide useful physiological insights into T2DM in PLHIV and ART.
There is a need for the development and implementation of a systematic screening plan for hyperglycemia using point of care devices in patients initiating DTG based regimen [26]. This can lead to early detection in patients with risk factors for T2DM and alternate regimen considered for patients assessed to be at high risk for T2DM [16].
Our study had limitations. Some of these include the design being observational and could possibly be exposed to bias or confounding introduced by patient self-reporting. We however cross-referenced information they provided from patient records to reduce the risk of bias. Again, family history of diabetes, dietary and lifestyle characteristics of patients were not assessed though they have an impact of the outcome of interest. The study determined fasting blood sugar level by assessing capillary blood using glucometers and did not assess plasma glucose. We tried to reduce the risk by using the same brand of glucometer across all sites. In addition, the point of care tests would be easier to implement if these findings are to be translated into practice. We also did not test for Hemoglobin A1c (HbA1c) levels as part of confirmation of T2DM which would have provided a comprehensive assessment of glycemic control over time. In our general population, we do not routinely use HBA1c for diagnosis of T2DM and the same was done in this observational cohort. Detections in blood sugar fluctuations would have been more robust if patients’ capacity were enhanced to frequently self-monitor, record and report blood sugar levels in-between study visits.
In spite of the limitations, the study was performed on a large representative population in Ghana, West Africa, adding on to diversity of knowledge on DTG and hyperglycemia within sub-Saharan Africa. The longitudinal nature and having an established baseline glycemic levels adds to the robustness of the study findings.


留言 (0)