
記住我


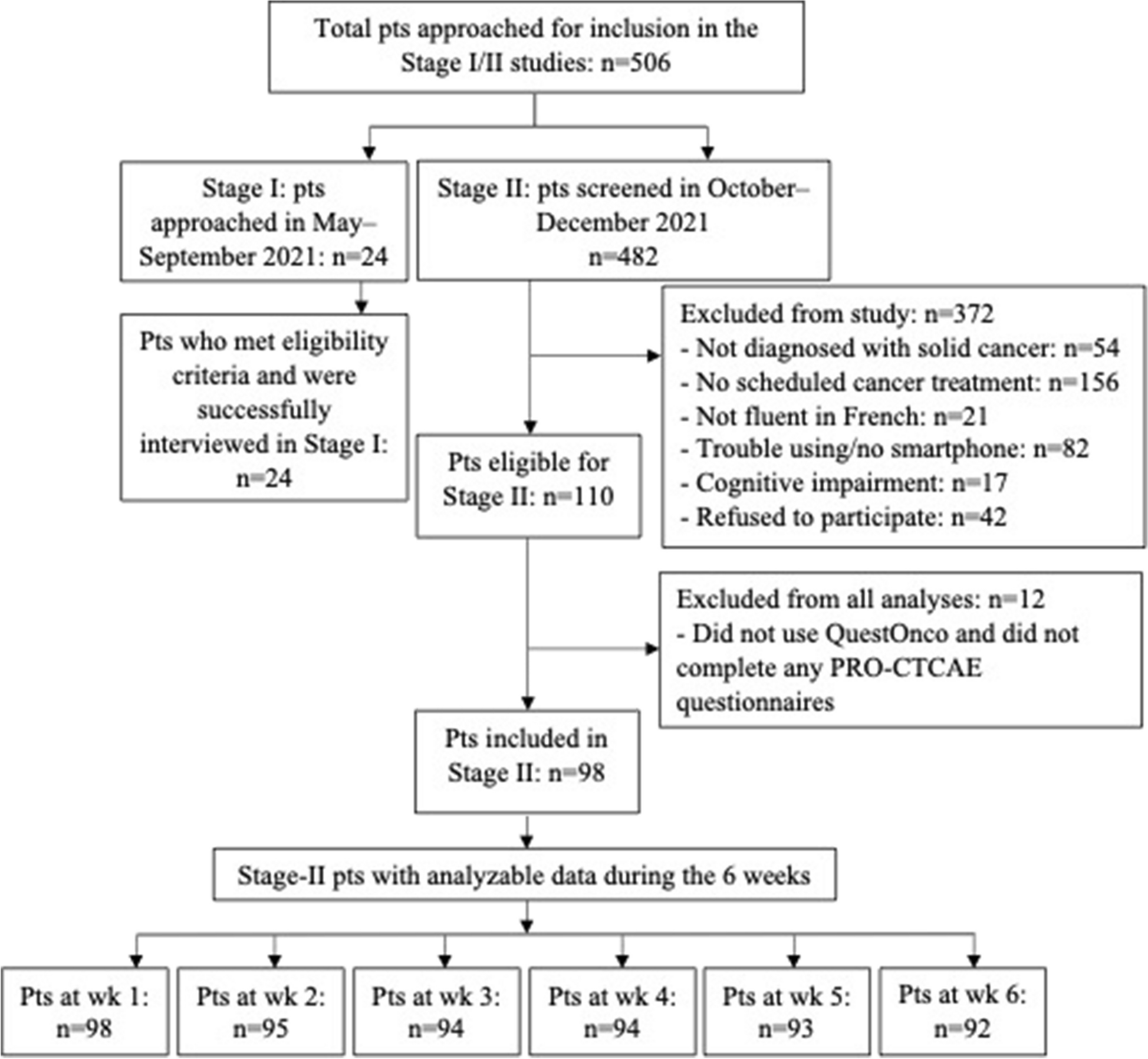
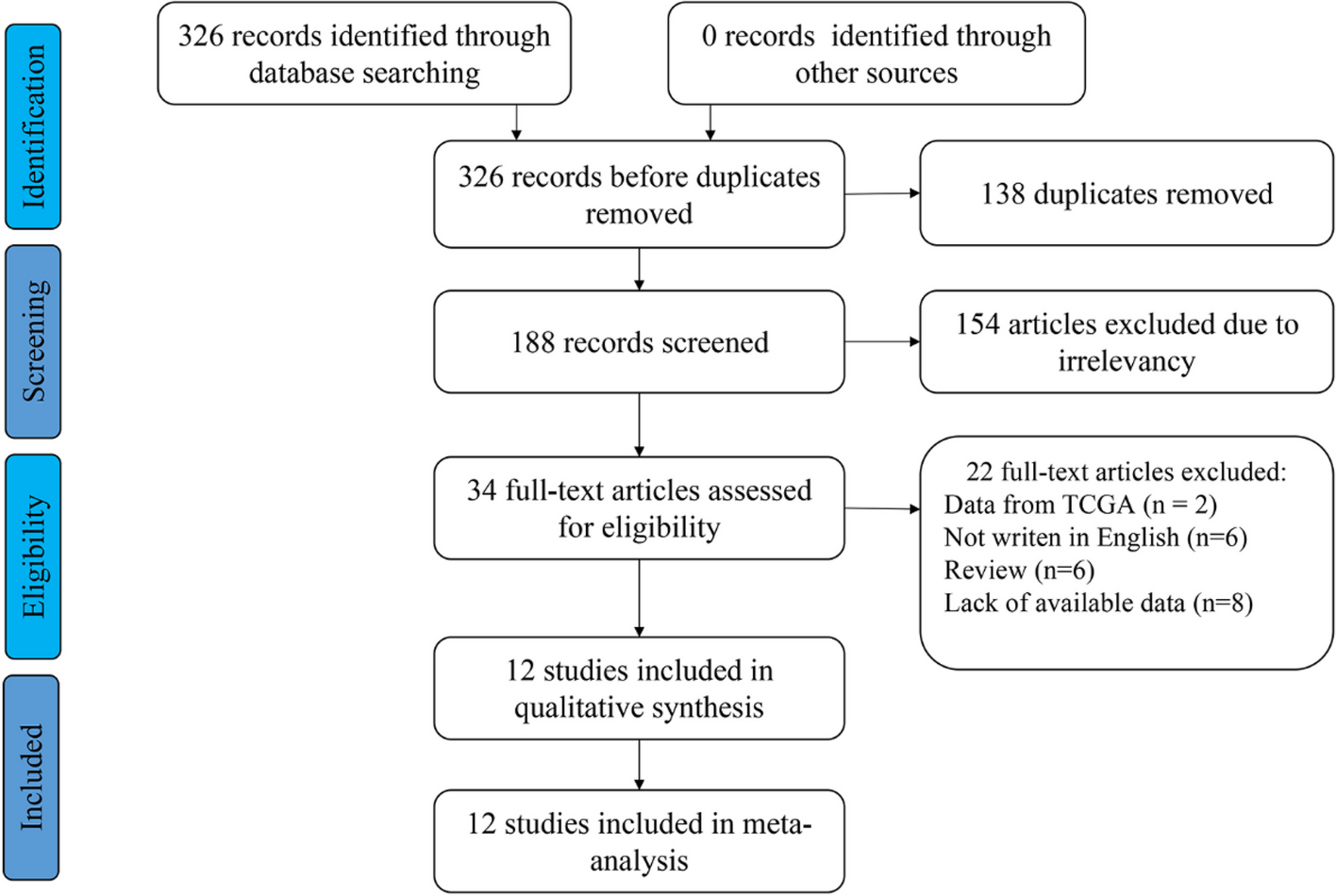

The flow diagram of this study is presented in Fig. 1. The baseline clinical characteristics information of 356 non-metastatic PCa patients were listed in Table 1. The mean (standard deviation (SD)) age of all patients was 69.19 (6.46) years. The Initial PSA at diagnosis of all patients was 21.57 (6.20–97.04) ng/ml. The number of patients with ISUP group ≤ 3 was 194 (54.49%), and the number of patients with ISUP group > 3 was 162 (45.51%). There were no significant differences observed in Age, BMI, initial PSA level, ISUP grading group, Lymph nodes metastasis, Positive surgical margin, Peri-prostatic fat involvement, Perineal invasion, Lymphovascular invasion as well as BCR rates between the training group, validation group, and testing group.
Fig. 1
Flow diagram of this study
Table 1 Baseline characteristics of 356 PCa patientsThe median follow-up duration in the study was 51.07 months, ranging from 46.48 to 55.67 months. The number of patients who experienced BCR was 121 (33.98%). During the follow-up of the 121 patients who experienced BCR, eleven (9.09%) patients developed local recurrences. Of these, eight patients received salvage radiotherapy, and 3 patient received salvage radiotherapy combined with androgen deprivation therapy (ADT) (leuprorelin, 3.75 mg every four weeks). Additionally, fifteen (12.40%) patients developed distant metastases. Of these, ten patients were treated with ADT combined with abiraterone acetate (1000 mg daily) plus prednisone (5 mg daily) or enzalutamide (160 mg daily), and 5 patients were treated with ADT combined with chemotherapy (docetaxel, dose of 75 mg/sqm every three weeks, six cycles).
Identification of periprostatic fat and intratumoral radiomics featureWe extracted 2632 radiomics features form the periprostatic fat ROI (1316 radiomics features from ADC and 1316 radiomics features from T2WI) and intratumoral ROI (1316 radiomics features from ADC and 1316 radiomics features from T2WI), respectively. After ICC analysis, the count of periprostatic fat features decreased to 1937 (899 features from ADC and 1038 features from T2WI), while the count of intratumoral features decreased to 1831 (932 features from ADC and 899 features from T2WI). The remaining features were ranked by the mRMR algorithm to retain the top 40 periprostatic fat and intratumoral radiomics features for the construction of radiomic scores (Supplementary Table 3).
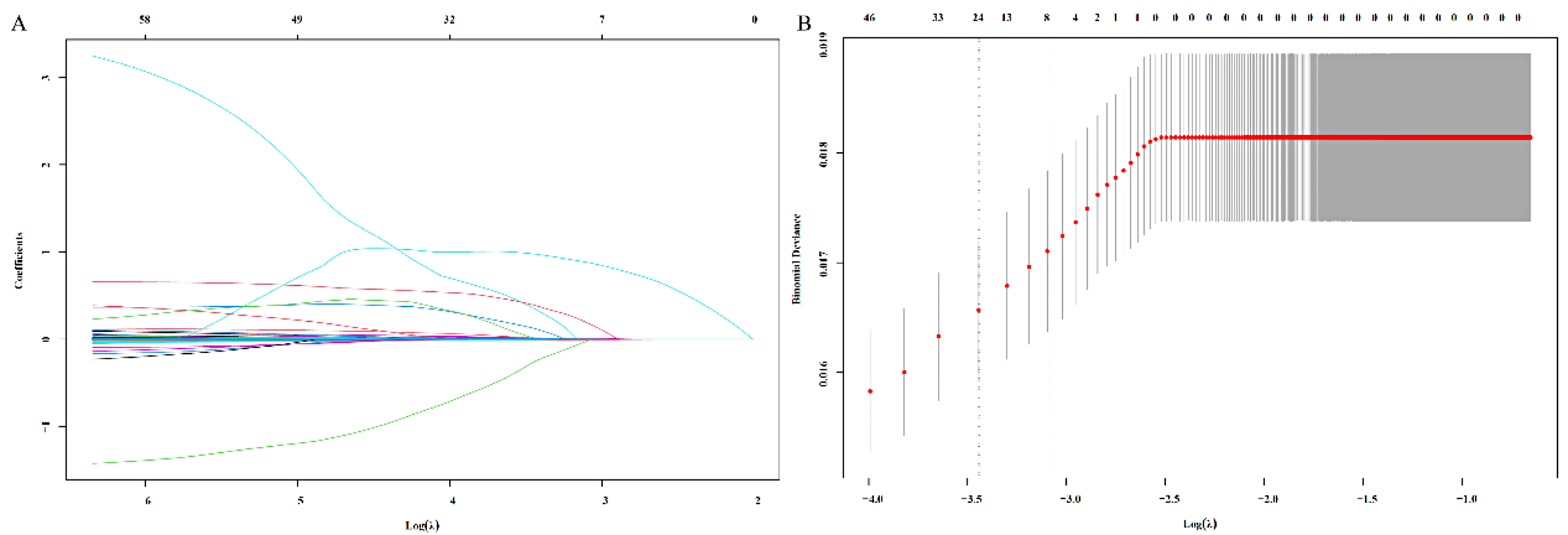
Construction and validation of radiomicsBy employing LASSO Cox regression analysis, we identified eight radiomics features for constructing the periprostatic fat radiomics score, six features for constructing the intratumoral radiomics score, and another eight features for constructing the periprostatic fat-intratumoral radiomics score (Table 2; Fig. 2). The formula for the radiomics scores was as following.
$$\mathrm\;\mathrm\;=\sum\limits_^n\left(\mathrm\;}_i\ast\;}_i\right)$$
Table 2 LASSO COX regression analyses constructing three radiomics scores for predicting bRFS in patient with non-metastatic PCa receiving RP treatmentFig. 2
LASSO Cox regression analyses of three radiomics models. A, C, E The partial likelihood deviance was plotted versus log (λ). The y-axis indicates the partial likelihood deviance, while the lower x-axis indicates the log (λ) and the upper x-axis represents the average number of predictors. Dotted vertical lines were drawn at the optimal values using the minimum criteria and 1 standard error of the minimum criteria. The tuning parameter (λ) was selected in the LASSO model via 10-fold cross-validation based on minimum criteria. A The lambda.min used in the LASSO algorithm for the periprostatic fat radiomics score is 0.05181153; B The lambda.min used in the LASSO algorithm for the intratumoral radiomics score is 0.08555169; C The lambda.min used in the LASSO algorithm for the periprostatic fat-intratumoral radiomics score is 0.07075123. The coefficients (y-axis) were plotted against log (lambda) and (B) 8 features with nonzero coefficients were selected to build periprostatic fat radiomics model, D 6 features with nonzero coefficients were selected to build intratumoral radiomics model, F and 8 features with nonzero coefficients were selected to build periprostatic fat-intratumoral radiomics model. LASSO, the Least absolute shrinkage and selection operator
The risk score of each patient was calculated based on radiomics scores. All patients were classified into high-risk and low-risk groups according to the median risk score. Kaplan-Meier analysis conducted in training and validation groups were illustrated in Fig. 3. Survival analysis demonstrated that the bRFS of patients with high-risk was significantly decreased compared with that of patients with low-risk.
Fig. 3
Kaplan-Meier curve analyses of three radiomics models. A periprostatic fat radiomics model in the training group. B periprostatic fat radiomics model in the validation group. C intratumoral radiomics model in the training group. D intratumoral radiomics model in the validation group. I periprostatic fat-intratumoral radiomics model in the training group. F periprostatic fat-intratumoral radiomics model in the validation group
The ROC curves of the three models in the training and validation groups were shown in Fig. 4. The AUCs of the periprostatic fat radiomics model in the training group were 0.901 (95%CI, 0.817–0.982), 0.856 (95%CI, 0.741–0.923), 0.833 (95%CI, 0.687–0.921) at 1-year, 3-years and 5-years bRFS in training cohort (Fig. 4A), and the AUCs in the validation group were 0.823 (95%CI, 0.663–0.965), 0.796 (95%CI, 0.656–0.943), 0.771 (95%CI, 0.642–0.905) at 1-year, 3-years and 5-years bRFS (Fig. 4B). The AUCs of the intratumoral radiomics model in the training group were 0.803 (95%CI, 0.640–0.889), 0.778 (95%CI, 0.606–0.865), 0.758 (95%CI, 0.600–0.827) at 1-year, 3-years and 5-years (Fig. 4C), and the AUCs in the validation group were 0.858 (0.731–0.961), 0.754 (95%CI, 0.624–0.895), 0.702 (95%CI, 0.610–0.863) at 1-year, 3-years and 5-years (Fig. 4D). The AUCs of the periprostatic fat-intratumoral radiomics model in the training group were 0.921 (95%CI, 0.857–0.981), 0.875 (95%CI, 0.763–0.950), 0.854 (95%CI, 0.706–0.923) at 1-year, 3-years and 5-years (Fig. 4E), and the AUCs in the validation group were 0.858 (95%CI, 0.731–0.961), 0.754 (95%CI, 0.624–0.895), 0.702 (95%CI, 0.610–0.863) for 1-year, 3-years and 5-years bRFS (Fig. 4F).
Fig. 4
ROC curve analyses of one-year, three-years, five-years for bRFS of three radiomics models. A periprostatic fat radiomics model in the training group. B periprostatic fat radiomics model in the validation group. C intratumoral radiomics model in the training group. D intratumoral radiomics model in the validation group. I periprostatic fat-intratumoral radiomics model in the training group. F periprostatic fat-intratumoral radiomics model in the validation group. ROC, the receiver operating characteristic. bRFS, biochemical recurrence-free survival
The performance of each radiomics score was compared and summarized in Table 3. The periprostatic fat-intratumoral radiomics score achieved the highest AUC values for 1-year (AUC: 0.921, 95% CI: 0.857–0.981), 3-year (AUC: 0.875, 95% CI: 0.763–0.950), and 5-year (AUC: 0.854, 95% CI: 0.706–0.923) bRFS. The periprostatic fat-intratumoral radiomics score showed a significant improvement in predicting 1-year (AUC: 0.803; 95%CI: 0.640–0.889; P = 0.010) and 3-year bRFS (AUC: 0.778; 95%CI: 0.606–0.865; P = 0.017) compared to the intratumoral radiomics score. Whereas periprostatic fat radiomics model and intratumoral radiomics model demonstrated similar performance for 1-year (AUC: 0.901, 95% CI: 0.817–0.982; P = 0.051), 3-year (AUC: 0.856, 95% CI: 0.741–0.923; P = 0.136), and 5-year (AUC: 0.833, 95% CI: 0.687–0.921; P = 0.241) bRFS. Therefore, the periprostatic fat-intratumoral radiomics model was identified for further analysis.
Table 3 Comparing ROC curves of three radiomics scoresConstruction and validation of clinical modelUnivariable Cox regression analysis revealed that initial PSA at diagnosis (P = 0.05; HR = 1.024; 95%CI, 1.007–1.042), pathological T stage (P = 0.002; HR = 2.780; 95%CI, 1.438–5.374), ISUP grading group of surgical specimens (P < 0.001; HR = 3.466; 95%CI, 1.699–7.069), positive surgical margin (P < 0.001; HR = 4.401; 95%CI, 2.215–8.744) were associated with bRFS of PCa patients receiving RP treatment (Table 4). A clinical model was constructed using multivariate Cox regression analysis based on the results obtained from univariable Cox regression analysis (Fig. 5A).
Table 4 Univariate and multivariate Cox regression analyses exploring prognostic factors for predicting bRFS in patients with non-metastatic PCa receiving RP treatmentFig. 5
Construction and validation of clinical model. A multivariate Cox regression analysis of clinical characteristics based on univariable Cox regression analysis. B ROC curve analyses of one-year, three-years, five-years for bRFS of clinical model in the training group. C ROC curve analyses of one-year, three-years, five-years for bRFS of clinical model in the validation group. D Kaplan-Meier curve analyses of clinical model in the training group. I Kaplan-Meier curve analyses of clinical model in the validation group. ROC, the receiver operating characteristic. bRFS, biochemical recurrence-free survival
The risk score of each patient was calculated based on the clinical risk scores. All patients were categorized into high-risk and low-risk groups according to the median risk score. As illustrated in Fig. 5B and E. Kaplan-Meier analysis revealed that patients with a high-risk profile experienced significantly shorter bRFS in comparison to those in the low-risk group (P < 0.001), with an AUC of 0.839, 0.776, and 0.819 for 1-year, 3-year, and 5-year bRFS, respectively, in the training group. And in the validation group, high-risk patients had significantly shorter bRFS than low-risk patients (P = 0.007), with an AUC of 0.838, 0.761, and 0.810 for 1-year, 3-year, and 5-year bRFS, respectively.
Development and validation of combined radiomics-clinical nomogramBased on the periprostatic fat-intratumoral radiomics score and significant clinical characteristics, a combined radiomics-clinical nomogram for predicting bRFS of PCa patients was developed by using multivariate Cox regression analysis (Fig. 6). The AUCs of radiomics-clinical nomogram in the training group were 0.944 (95%CI, 0.912–0.990), 0.864 (95%CI, 0.772–0.969), 0.907 (95%CI, 0.836–0.982) at 1-year, 3-years and 5-years bRFS in training cohort (Fig. 7A), the AUCs in the validation group were 0.875 (95%CI, 0.750–0.998), 0.814 (95%CI, 0.676–0.953), 0.869 (95%CI, 0.712–0.997) at 1-year, 3-years and 5-years bRFS (Fig. 7C), and AUCs in the testing group were 0.815 (95%CI, 0.664–0.921), 0.729 (95%CI, 0.641–0.883), 0.854 (95%CI, 0.702–0.913) (Fig. 7E). Kaplan-Meier analysis revealed that patients with high-risk experienced significantly shorter bRFS in comparison to those in the low-risk group (P < 0.001) in the training group, validation group, and testing group (Fig. 7B, D and F). In addition, the calibration curves of the radiomics-clinical nomogram revealed that the predicted and observed survival probability of 1-years, 3-year and 5-year bRFS had high degree of consistency in the training group, validation group, and testing group (Fig. 8).
Fig. 6
The radiomics-clinical nomogram. A Nomogram for predicting one-year, three-years, five-years bRFS of PCa patients receiving RP treatment. B How to use: (1) locate the patient’s radiomic score, Pathological T stage, ISUP grading group, Positivity surgical margin and then draw a straight line on the top dot axis to obtain the corresponding score; (2) sum the scores obtained; (3) find the final sum on the total point axis and draw a straight line down to assess the risk of bRFS in patients with PCa. bRFS, biochemical recurrence-free survival. PCa, prostate cancer
Fig. 7
ROC curve and Kaplan-Meier curve analyses of the radiomics-clinical nomogram. ROC curve analyses of one-year, three-years, five-years for bRFS of combined radiomics-clinical nomogram in the training group (A), validation group (C), and testing group I. Kaplan-Meier curve analyses of radiomics-clinical nomogram in the training group (B), validation group (D), and testing group (F). ROC, the receiver operating characteristic. bRFS, biochemical recurrence-free survival. PCa, prostate cancer. RP, radical prostatectomy
Fig. 8
Calibration curves of the combined radiomics-clinical nomogram. A-C Calibration curves of the combined radiomics-clinical nomogram for one-year, three-years, five-years bRFS in the training group. D-F Calibration curves of the combined radiomics-clinical nomogram for one-year, three-years, five-years bRFS in the validation group. G-I Calibration curves of the combined radiomics-clinical nomogram for one-year, three-years, five-years bRFS in the validation group. bRFS, biochemical recurrence-free survival
The comparison of ROC curves for the optimal radiomics score, the clinical model, and the radiomics-clinical nomogram was presented in Table 5. The radiomics-clinical nomogram demonstrated the highest AUC values for 1-year bRFS (AUC: 0.944, 95%CI: 0.912–0.990) and 5-year bRFS (AUC: 0.907, 95%CI: 0.836–0.982) in the training group. Furthermore, the radiomics-clinical nomogram exhibited a substantial improvement compared to clinical model in predicting 1-year (AUC: 0.944; 95%CI, 0.912–0.990 vs. AUC: 0.839; 95%CI, 0.661–0.928; P = 0.009), 3-year (AUC: 0.864; 95%CI, 0.772–0.969 vs. AUC: 0.776; 95%CI, 0.602–0.872; P = 0.008), and 5-year bRFS (AUC: 0.907; 95%CI, 0.836–0.982 vs. AUC: 0.819; 95%CI, 0.687–0.915; P = 0.027) respectively. Additionally, no statistically significant disparity was observed between the performance of the periprostatic fat-intratumoral radiomics score and the clinical model.
Table 5 Comparing ROC curves of optimal radiomics model, clinical model and radiomics-clinical nomogram
留言 (0)