Study population
This prospective cohort study made use of a nationally representative sample from the National Health and Nutrition Examination Survey (NHANES). The Centers for Disease Control and Prevention (CDC) ascertained causes and time to death information by linking eligible NHANES participants to the National Death Index. The study, which combines questionnaire surveys, laboratory examinations and physical examinations, has been conducted biennially since 1999, focusing on various population groups or health issues. The Institutional Review Board of the National Center for Health Statistics granted approval for the NHANES study, with participants giving their written informed consent.
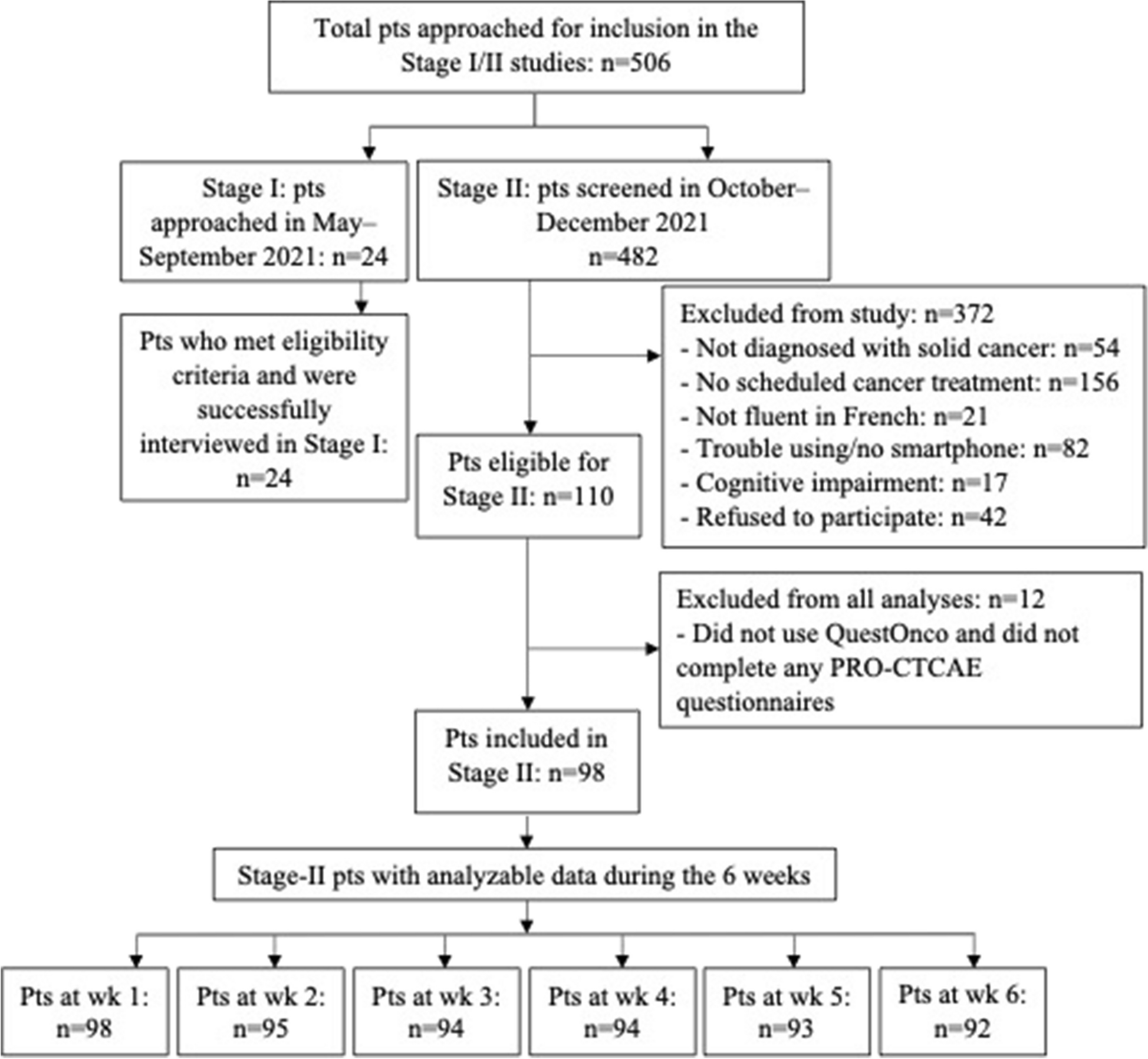
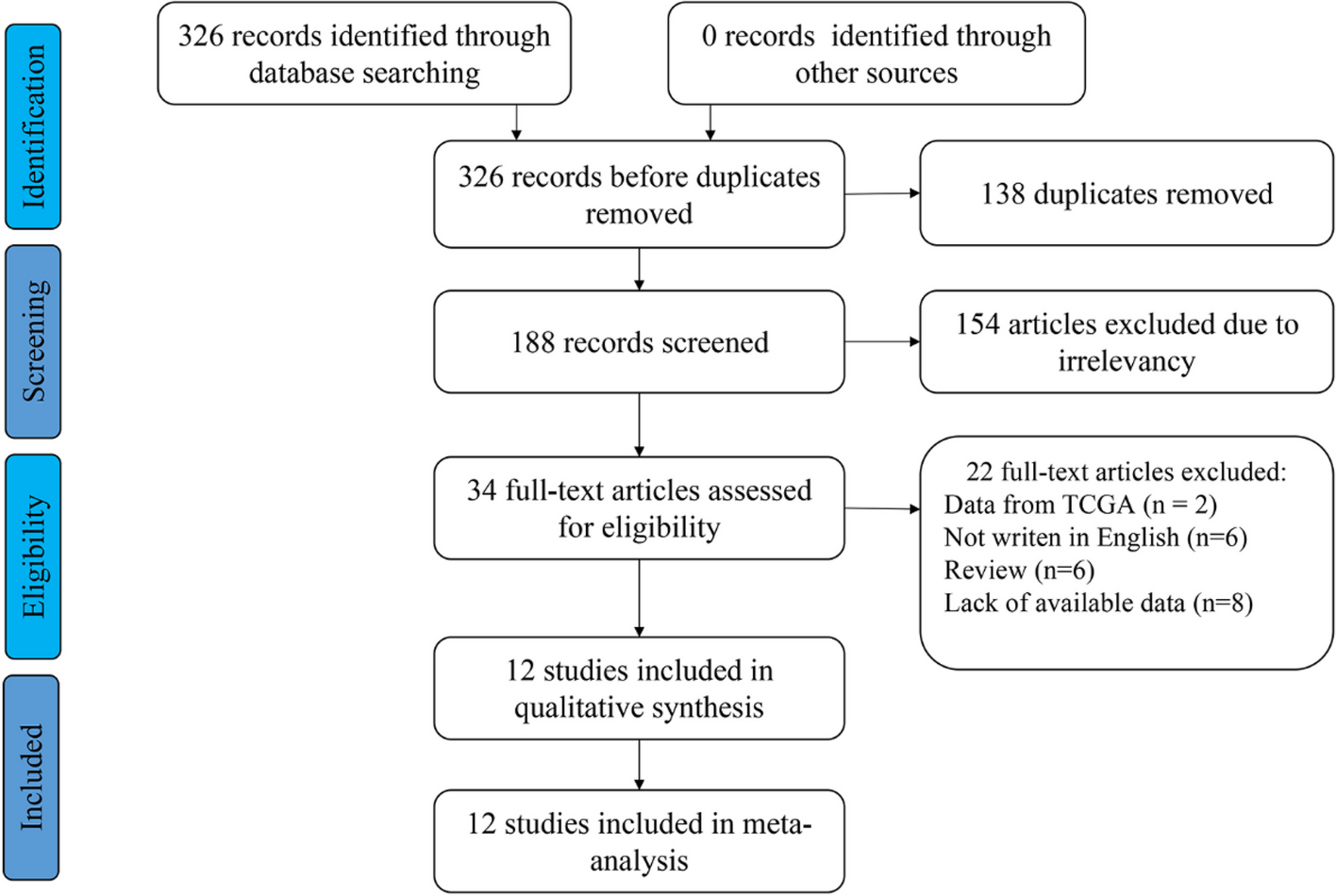
Initially, a total of 3,782 cancer survivors were recruited across seven 2-year NHANES survey cycles from 2005–2006, 2007–2008, 2009–2010, 2011–2012, 2013–2014, 2015–2016, and 2017–2018. Participants were queried, "Have you ever been told by a doctor or other health professional that you had cancer or a malignancy of any kind?" Those who answered affirmatively were defined as cancer survivors from diagnosis. From these participants, individuals under the age of 40 (n = 252), missing ALI-related data (n = 539), lacking sleep quality data (n = 915), or missing any covariate-related information (n = 168) were excluded from the analysis. The final analysis included 1908 patients (eFigure 1). The count of cancer survivors, segmented by gender and type of cancer, is provided in eTable 1.
Assessment of ALI and sleep quality
The ALI was calculated with the formula: ALI = BMI × Alb/NLR, where BMI was determined by dividing weight in kilograms by the square of height in meters, Alb stood for serum albumin levels measured in grams per deciliter, and NLR was the ratio of absolute neutrophil count to absolute lymphocyte count. ALI was categorized into two groups: Low (≤ 53.2) and High (> 53.2).
Sleep quality-related data encompassed sleep duration, trouble sleeping, and sleep disorders [21]. Sleep duration was defined by the response to the question, "On workdays or school days, how many hours of sleep do you usually get at night?" Participants were queried, "Have you ever told a doctor or other health professional that you have trouble sleeping?" Those who answered "yes" were considered to have trouble sleeping. Additionally, participants were queried, "Have you ever been told by a doctor or other health professional that you have a sleep disorder?" Those who answered "yes" were regarded as having a sleep disorder.
To explore the potential mediating role of ALI and sleep duration on all-cause mortality, we performed a mediating analysis, focusing on the role of BMI and NLR. Use the Mediation package in R software version 4.3.1 for causal step analysis.
Covariate definitions
In this study, we considered the following variables as covariates: gender, age, race/ethnicity, BMI, family poverty income ratio, level of education and age at first cancer diagnosis. The categories used to classify race/ethnicity were non-Hispanic white, non-Hispanic black, other Hispanic, Mexican American, and other race/ethnicity. BMI was divided into three groups: < 25, 25.0 to 29.9, and ≥ 30. The family poverty income ratio was categorized into three groups: < 1.3, 1.3 to ≤ 3.5, and ≥ 3.5. For educational levels, the categories were less than high school (ninth grade or less, ninth to eleventh grade including twelfth grade without a diploma), high school (high school diploma or General Equivalency Diploma, some college or associate's degree), and beyond high school (college graduate or higher). In addition, we grouped cancer types into digestive, genitourinary, skin, breast, and other cancers to assess the association of ALI levels and sleep quality with mortality in different cancer types.
Mortality definitions
The primary outcome of this study was centered on all-cause mortality, with secondary outcomes addressing mortality specific to cancer and mortality unrelated to cancer. All-cause mortality encompassed deaths from any cause, cancer-specific mortality was determined by the UCOD_LEADING codes for Malignant neoplasms (019–043), and deaths from causes other than cancer were categorized as non-cancer-specific mortality.
Statistical analysis
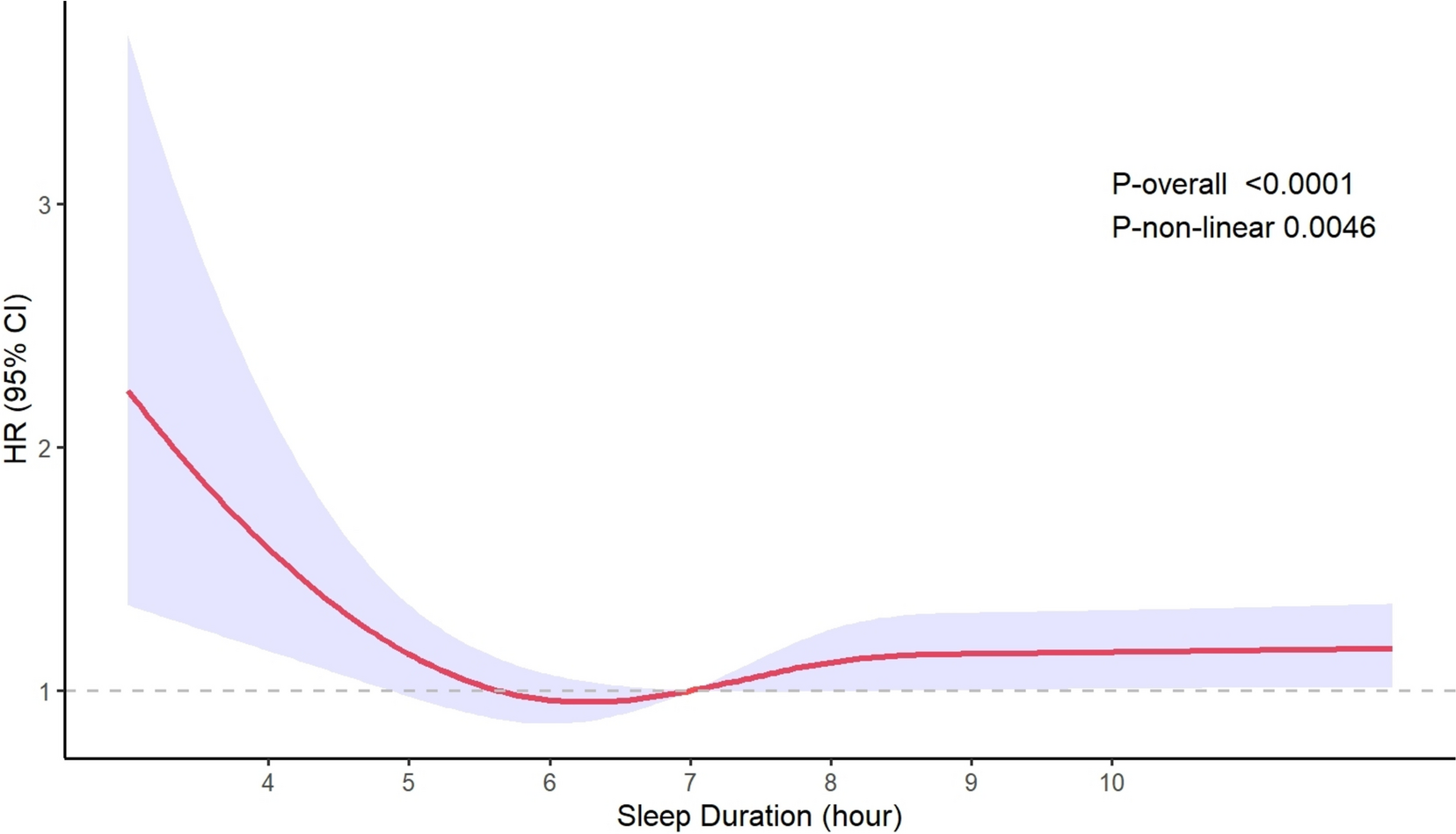
Adhering to the NHANES analysis guidelines, this study integrated sample weights, clustering, and stratification in its analyses to precisely estimate variance and guarantee that the findings are nationally representative of cancer survivors in the United States. Baseline characteristics provided insights into different levels of the ALI and the quality of sleep. Restricted cubic splines (RCS) were used to illustrate the non-linear relationship between ALI or sleep duration and the HR for all-cause and non-cancer-specific mortality. We calculated the best cutoff value for ALI on the ROC curve, corresponding to the point with the highest Youden index, where both sensitivity (true positive rate) and specificity (1-false positive rate) reach their maximum simultaneously. To assess the independent association between ALI and sleep quality with all-cause, cancer-specific, and non-cancer mortality, weighted multivariable Cox proportional hazards regression models were used to calculate Hazard ratio (HR) and 95% Confidence interval (CI). The final multivariable models were adjusted for factors including gender, age, race and ethnicity, BMI, family poverty income ratio, education level, and age at first cancer diagnosis. To evaluate the combined impact of ALI and sleep quality on mortality risk, participants were categorized based on ALI and sleep quality, and weighted multivariable Cox proportional hazards regression models adjusted for the same set of covariates were utilized. In the analysis of cancer-specific and non-cancer-specific mortality, it is considered that both short and long sleep durations were associated with an increased risk of mortality. Sleep duration was simplified into non-standard sleep duration (< 7 & > 9 h) and standard sleep duration (7 to 9 h). All analyses were conducted using a two-sided approach, with an alpha significance level set at 0.05. All statistical analyses were performed using R version 4.3.1.




留言 (0)