
記住我




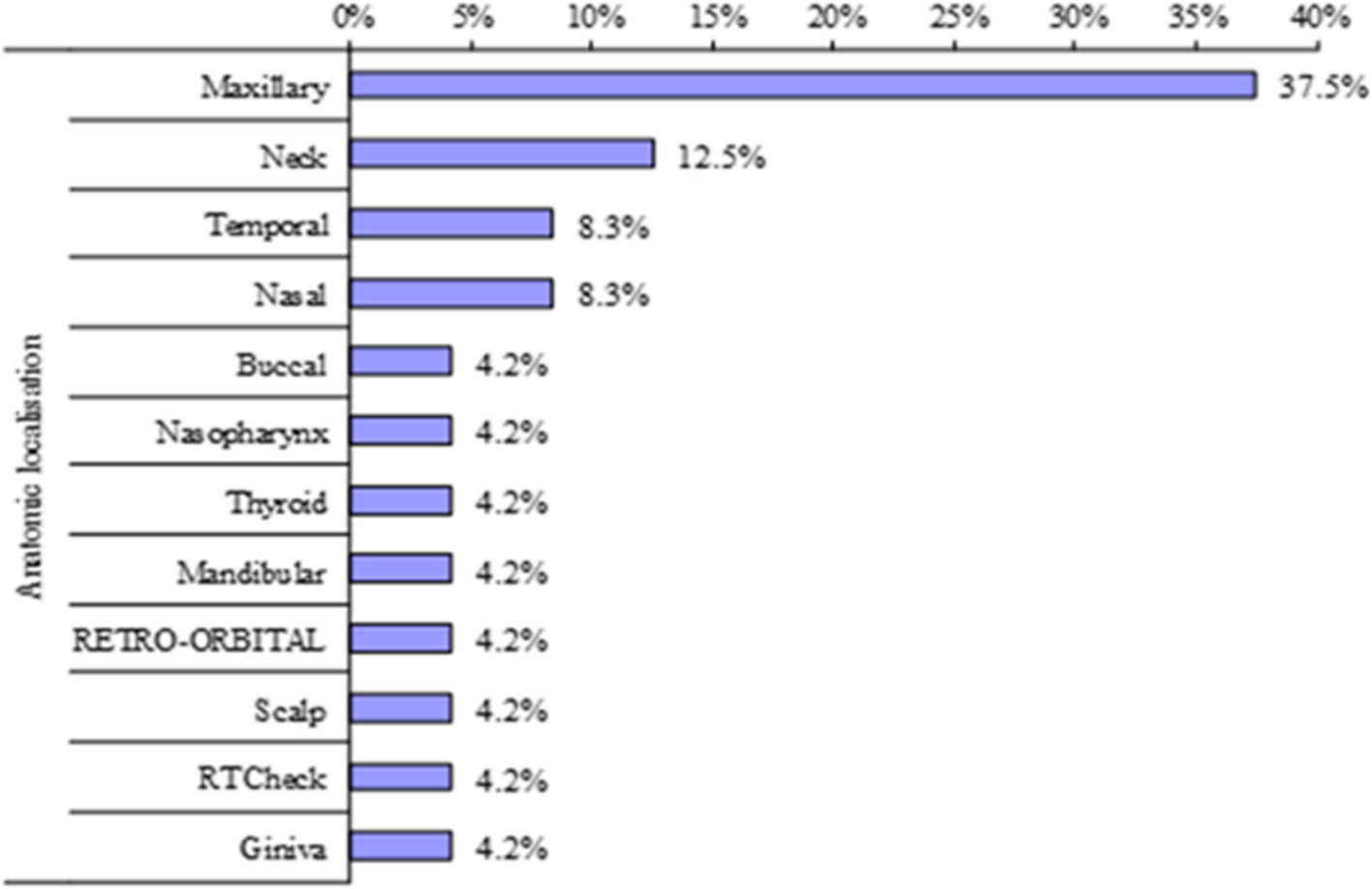

Twenty-four patients were enrolled with mean age 37.7 years (range 17–80). Female gender was predominant (15/24) representing 62.5% (Table 1). The commonest site was maxilla as 9 patients presented with maxillary lesion (37.5%) divided as 3 maxillary osteosarcoma and 6 maxillary soft tissue sarcomas. Neck was the second common presented site (12.5%) (Fig. 1).
Table 1 Analytical data related to patients’ personal history, tumor site, diagnosis, and pathological typeFig. 1
Shows anatomical sites of tumor presentation
Rhabdomyosarcoma and osteosarcoma were the most common pathological subtypes with equal presentation by 4 patients for each (16.7%) (Fig. 2). Less common presentation of Dermatofibrosarcoma protuberans (DFS), angiosarcoma, synovial sarcoma and fibrosarcoma (8,3% for each).
Fig. 2
Shows pathological subtypes presentation
Regarding TNM staging, T2N0M0 was most common presenting stage (13 patients). T2-stage was the tumor stage in 54.2% of patients and less common T3- stage in 25% of patients. Twenty patients presented with negative LN affection 20/24 (83.3%). At presentation, 23/24 patients showed localized disease (95.8%), while 1/24 patient (4.2%) was metastatic to bone. Mitotic count score 1 was more common than score 2 (58.3% vs 41.7%). Fourteen patients’ tumor samples showed no tissue necrosis by pathological examination. Grade II had the upper hand by both TNM grading and FNCLCC grading (66.7%, 45.8% respectively) (Table 2).
Table 2 Analytical data related to tumor stage (TNM) and pathological gradingPrimary surgical treatment was done for 20 patients (83.33%) with R0 margin was achieved in 6 patients (25%), R1 margin in 11 patients (45.8%) and only 3 patients had R2 resected margins (12.5%). Radiotherapy was given as adjuvant treatment in 9/24 patients, as definitive in 2/24 and as palliative in one patient.
Chemotherapy was given in 5 patients as adjuvant chemotherapy and 3 patients received neoadjuvant chemotherapy. The main chemotherapy protocol used was VAC (vincristine, adriamycin, cyclophosphamide) as was given to 4 patients. Two patients received (cisplatin and adriamycin) combination protocol, one received (ifosfamide and adriamycin) combination protocol and one received VAC-IE (vincristine, adriamycin, cyclophosphamide alternating with ifosfamide, etoposide). Eight patients had local recurrence (8/20) and 3 systemic metastasis (3/23). By the end of the study, 17 patients were still alive (70.8%) (Table 3).
Table 3 Relapsed disease, site of relapse and palliative treatmentMean time to relapse (TTR) of studied patients was 39.117 months with 95% CI (26.708 to 51.526), mean time to local relapse was 41.76 months with 95% CI (29.561 to 53.962) while mean time to systemic relapse was 56.08 months with 95% CI (46.790 to 65.369) (Table 4).
Table 4 Shows estimated time to overall relapse, time to local relapse and time to systemic relapse of studied patientsRegarding overall survival (OS) of patients of our study, Mean OS was 47.223 months with 95% CI (36.668 to 57.778) (Table 5, Fig. 3). The tumor grade, necrosis, margin, and adjuvant chemotherapy showed a trend to improve the OS but did not reach statistical significance, which may be related to the small sample size, and the 5-year OS was 65.4%. So, correlative survival analysis between different clinic-pathological factor and survival was difficult.
Table 5 Shows estimated overall survival (OS) of studied patientsFig. 3
Overall survival curve of studied patients according to Kaplan Mayer analysis
留言 (0)