
記住我

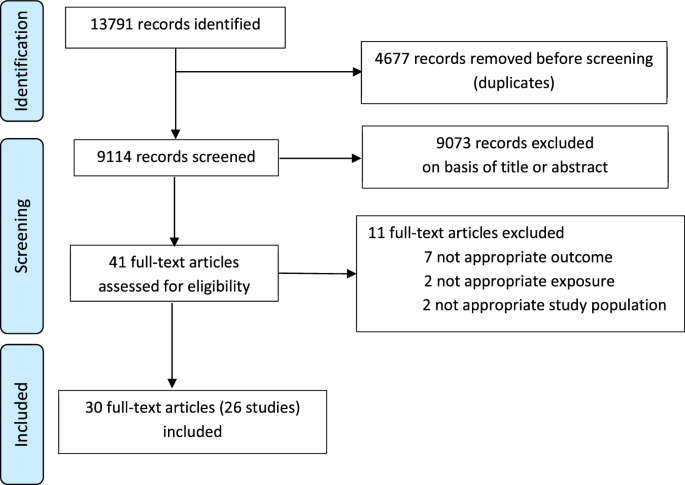
Of 3238 volunteers screened 2366 were enrolled and randomized 1:1 to the two study groups (Fig. 1). Demographics of the two groups were balanced with the same median ages (52 years) and approximately equal numbers of men and women, with similar baseline characteristics (height, weight, BMI) and equal stratification of the 18–59-year-olds into healthy and at-risk groups (Table 1).
Fig. 1: Study flow chart.
Numbers of volunteers screened and participants enrolled in ARCT-154 and ChAdOx1-S groups at each study milestone and analysis sets are displayed. mITT modified intention-to-treat, SAS safety analysis set.
Table 1 Demographics of the randomized and vaccinated study populationSafetyThere were four deaths, all in the ChAdOx1-S group; reported during the safety follow-up period to Day 394 which were due to Non-Hodgkin’s lymphoma, gastrointestinal hemorrhage, esophageal carcinoma and a cerebrovascular accident (Table 2). The deaths were not considered to be related to study vaccination. There were 170 participants who reported at least one serious adverse event (SAE), 83 (7.0%) in 1186 ARCT-154 vaccinees and 87 (7.4%) in 1180 ChAdOx1-S vaccinees, including 8 and 9 cases of COVID-19 in each study group, respectively (Table 2). Most SAEs were not considered to be related to vaccination, but cases of angina pectoris, polyarthritis and cerebral infarction in the ARCT-154 group, and angina pectoris, chest pain and two cases of headache in the ChAdOx1-S group were considered to be related to vaccination by the investigator. Of these, two SAEs in ARCT-154 recipients (polyarthritis and cerebral infarction) and one in a ChAdOx1-S recipient (angina pectoris), resulted in their discontinuation from the study vaccinations. Medically-attended adverse events were reported by similar proportions of study participants in both vaccine groups, 461 (38.9%) and 496 (42.0%) of ARCT-154 and ChAdOx1-S groups, but most were not related to vaccination (Table 2).
Table 2 Overall adverse events in the Safety Set and in the two age groups after each vaccinationAfter the first dose, the reactogenicities of the two vaccines were similar, with local reactions being reported by 467 (39.5%) of 1182 ARCT-154 recipients and 416 (35.4%) of the 1176 ChAdOx1-S vaccinees in the Safety set who provided data (Table 2). These local reactions mainly consisted of mild pain or tenderness at the injection site (Fig. 2), which resolved within 1–2 days. Local reactions were less frequent in both groups after the second dose, reported by 286 (24.9%) of 1150 and 183 (15.9%) of 1149 ARCT-154 and ChAdOx1-S groups (Table 2), and still consisted mainly of transient mild pain or tenderness. The frequency of severe local solicited reactions after the first or second dose was 0.1% (1/1182) in the ARCT-154 group and 0.1% (1/1176) in the ChAdOx1-S group.
Fig. 2: Solicited reactogenicity.
The percentages of each study group reporting the solicited local reactions and systemic adverse events are displayed according to severity.
After the first dose, systemic solicited adverse events occurred in 638 (54.0%) of 1182 ARCT-154 vaccinees and 657 (55.9%) of 1176 ChAdOx1-S vaccinees. Incidence decreased to 477 (41.5%) of 1150 and 331 (28.8%) of 1149 after the second dose (Table 2). The most frequent systemic solicited adverse events were fatigue, headache, chills, and arthralgia after either dose (Fig. 2). Frequencies of severe systemic solicited AEs were similar after the first or the second doses of ARCT-154 (3.0% [35/1182]) and ChAdOx1 (3.7% [44/1176]). Solicited systemic AEs were transient, generally resolved within two days after dosing, and were similar in duration in ARCT-154 and the ChAdOx1-S groups. There were no meaningful differences in frequency or severity of adverse events observed between younger (18–59 years) and older (≥60 years) age groups, except for a lower frequency of solicited adverse reactions in older participants.
ImmunogenicityImmunogenicity assessment was performed in 917 randomly selected study participants of the immunogenicity analysis subset (IAS), 455 in the ARCT-154 group and 462 in the ChAdOx1 group, who received both study vaccinations and provided blood samples at all 5 time points (Days 1, 29, 57, 211 and 394). On Day 1, all but three participants, all in the ARCT-154 group, were negative for antibodies against the SARS-CoV-2 nucleocapsid protein (anti-N-protein), indicating no recent SARS-CoV-2 infections (Table 1). During the study period, 96 of 455 (21.1%) and 115 of 462 (24.9%) participants from the ARCT-154 and ChAdOx1-S IA subsets, respectively, reported virologically confirmed COVID-19 disease and by Day 394, only 100 of 455 (22.0%) and 76 of 462 (16.5%) participants in the ARCT-154 and ChAdOx1-S subsets, respectively, were still anti-N-protein negative (Supplementary Table 1). A further 31/100 (31%) and 23/76 (30.3%) of the individuals in the ARCT-154 and ChAdOx1-s group received non-study COVID-19 vaccines between Days 211 and 394 so were excluded from the immunogenicity analyses. This subset of N-protein-negative participants at Days 1 and 394 with no symptomatic COVID-19 constituted the SARS-CoV-2-naive cohort.
Those who seroconverted from negative to positive for anti-N-protein antibodies between Days 1 and 394—352/452 (77.9%) in ARCT-154 and 386/462 (83.5%) in ChAdOx1-S groups—with or without symptomatic COVID-19, constituted the SARS-CoV-2-exposed cohort. We randomly selected 105 participants from each vaccine group in this SARS-CoV-2-exposed cohort for immunogenicity testing of whom 10 individuals in ARCT-154 group and 17 individuals in ChAdOx1-S group had received non-study COVID-19 vaccines and were excluded from the analysis for respective time points after these non-study vaccinations.
Levels of neutralizing antibodies were either very low or unmeasurable before vaccination in both SARS-CoV-2-naive and SARS-CoV-2-exposed cohorts with baseline GMTs approximately half the LLOQ of the assay (baseline <LLOQ was imputed to half LLOQ). Four weeks after the first vaccination of SARS-CoV-2-naive participants there were marked increases in neutralizing antibodies after either vaccine, with a higher response in the ARCT-154 group—the geometric mean-fold rise (GMFR) was 7.5 (95% CI: 6.0–9.4) compared with 3.2 (2.6–3.9) after ChAdOx1-S (Fig. 3, Supplementary Table 2A). Titers increased further after the second dose, achieving GMFR of 29.9 (24.6–36.2) in the ARCT-154 group vs. 11.0 (8.7–13.9) in the ChAdOx1-S group. The ratios of GMTs between ARCT-154 and ChAdOx1-S groups were 2.34 (95% CI: 1.71–3.21) on Day 29 and 2.70 (2.00–3.64) on Day 57. On Day 211, 6 months after the second vaccination, the GMT plateaued in these subsets with no natural exposure to SARS-CoV-2—126 (95% CI: 86.2–183) after ARCT-154 and 77.5 (48.3–124) after ChAdOx1-S (Fig. 3). In SARS-CoV-2-naive participants the GMT increased to 253 (153–416) by Day 394, one year after vaccination, in the ARCT-154 group but was unchanged at 68.4 (40.8–115) in the ChAdOx1-S group, giving an ARCT-154 vs. ChAdOx1-S GMT ratio of 3.70 (1.80–7.59) (Fig. 3). Non-inferiority criteria were met for ARCT-154 compared with ChAdOx1-S at all post-vaccination time points.
Fig. 3: Neutralizing antibody responses.
Geometric mean titers of neutralizing antibody responses against Wuhan-Hu1 strain measured by CPE-based microneutralization assay (1/dil) after doses 1 (Day 1) and 2 (Day 29) of ARCT-154 or ChAdOx1-S, in baseline anti-N-protein naive subjects, according to N-protein seropositivity status on Day 394. Chart shows geometric mean titers (95% CI) with n values for each time point, and table shows the GMT ratio between ARCT-154 and ChAdOx1-S groups and the geometric mean-fold rises at each time point (with 95% CI).
In the SARS-CoV-2-exposed cohort the immune response to the first vaccination was also higher in the ARCT-154 group than in the ChAdOx1 group with GMFR of 7.9 (95% CI: 6.2–10.0) and 5.1 (4.0–6.4), respectively, and the inter-group GMT ratio of 1.56 (95% CI: 1.13–2.17) (Fig. 3, Supplementary Table 2B). The GMTs increased further after the second dose with GMFRs of 34.2 and 15.4 in ARCT-154 and ChAdOx1-S groups on Day 57, a GMT ratio of 2.22 (95% CI: 1.61–3.07), and continued to increase in both groups, presumably due to natural exposure to SARS-CoV-2. On Days 211 and 394 the inter-group GMT ratios were 1.31 (95% CI: 0.80–2.14) and 1.87 (1.30–2.71).
Age of the participants had no impact on the immune responses in SARS-CoV-2-naive or exposed participants (Supplementary Fig. 1), with responses similar in those aged 18–59 years, or those aged 60 years or more. The effect of apparent SARS-CoV-2 infection was still observed, with a continuing increase in GMTs up to Day 394, while in SARS-CoV-2-naive participants the GMTs plateaued at Days 211 and 394.
We assessed cross-neutralizing antibodies against SARS-CoV-2 Delta, Omicron BA.2, XBB.1.5.6 and BA.2.86 subvariants in a subset of participants (n = 31) from the ARCT-154 group who met the following criteria: were anti-N-protein negative on Day 1, did not have a virologically confirmed COVID-19 infection during the study, and had not received other COVID-19 vaccines. On Day 57, GMTs of neutralizing antibodies against the Wuhan strain were 485 (95% CI: 347–678), 34 (22–52) against Delta strain, and 16 (12–21) against Omicron BA.2 (Supplementary Table 3). Titers of neutralizing antibodies against more recent Omicron subvariants XBB.1.5.6 and BA.2.86 were close to the assay LLOQ.
The majority of these participants, 81% (25 of 31), seroconverted for anti-N-protein antibodies at Day 394, indicating asymptomatic infection or exposure to SARS-CoV-2 (Supplementary Table 3). Such natural infection elicited a robust booster response in neutralizing antibodies against all tested variants, most prominently for Omicron BA.2 with GMT increasing from 15 (95% CI: 12–19) to 756 (483–1182), then Delta from 30 (20–45) to 399 (223–715), and Wuhan-Hu-1 from 453 (312–656) to 2982 (2028–4384). Smaller increases in antibody titers were observed for Omicron XBB.1.5.6 subvariant from 11 (10–13) to 81 (46–142) and for Omicron BA.2.86 from 10 (10–11) to 24 (17–35).
Efficacy assessmentOverall, 48 confirmed cases of COVID-19 were reported between Days 36 and 92, but this was followed by a significant surge in cases up to the end of the study by when there was a total of 480 cases. Of these, 450 cases occurred between Days 36 and 211, with a further 30 cases then occurring up to Day 394. No case of severe COVID-19 was reported by the investigators or identified during the blinded case reviews, but six participants with COVID-19 infections were hospitalized for isolation purposes. The most frequent clinical symptoms in participants with COVID-19 were cough (58.3%), fever/chills (50.4%), sore throat (40.2%), headache (36.0%) and fatigue (34.6%). No sequencing was performed in this part of the study to identify variants of SARS-CoV-2 but epidemiological data are available for the study period showing the main circulating SARS-CoV-2 strains were Omicron sub-lineages BA.2 and BA.5 (Supplementary Fig. 2) and occurrence of COVID-19 cases and associated deaths (Supplementary Fig. 3).
In mITT participants, 20 and 28 virologically confirmed COVID-19 cases were reported in ARCT-154 and ChAdOx1-S groups, respectively, from Day 36 to Day 92, the end of per-protocol efficacy surveillance in the previous Phase 1/2/3a/3b part of the study (Table 3, Fig. 4A). This equates to a relative vaccine efficacy (rVE) for ARCT-154 of 30.7% (95% CI: −23.0–61.0) over a period when predominant SARS-CoV-2 strains were Delta (B.1.617.2) and Omicron BA.1 variants (Supplementary Fig. 2). As monitoring in this phase 3c study continued, the confirmed cases increased to 205 and 245 in ARCT-154 and ChAdOx1-S groups, respectively, during six months post-vaccination (until Day 211) due to a new surge of COVID-19 cases caused by the Omicron BA.2 variant (Supplementary Fig. 2). During this period the positive difference in rVE in favor of ARCT-154 over ChAdOx1-S of 19.3% (95% CI: 2.8–32.9) persisted (Table 3, Fig. 4B). For the full one year of monitoring from Day 36 until Day 394, the totals of 218 and 262 cases reported in ARCT-154 and ChAdOx1-S groups gave a rVE of 19.8% (95% CI: 4.0–33.0) (Table 3). When analyzed according to age group there is a trend for the rVE of ARCT-154 vs. ChAdOx1-S to increase with age (Table 3), despite no age-dependent difference being observed in the immune response.
Table 3 Relative vaccine efficacies (rVE) of ARCT-154 vs. ChAdOx1-S against confirmed protocol-defined COVID-19 (mITT)Fig. 4: Cumulative incidence of COVID-19 cases.
Relative vaccine efficacy (rVE) of ARCT-154 vs. ChAdOx1-S vaccine against any severity of COVID-19 from Day 36 (one week after the second dose) up to Day 92 (A) and from Day 36 up to Day 211 (B).
留言 (0)