Data description
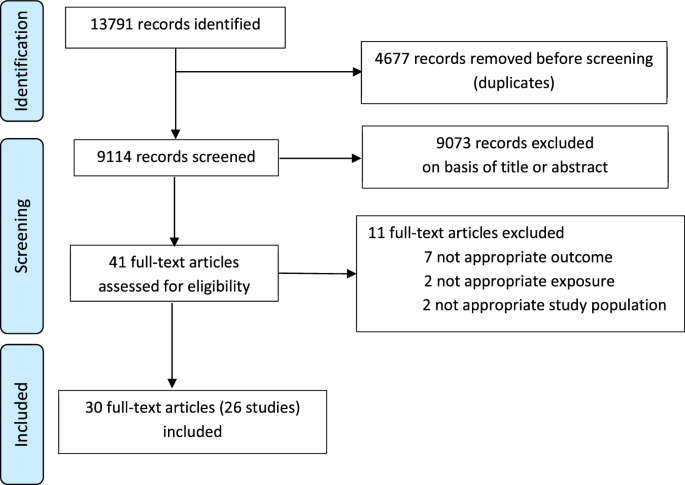
Surveillance for RVGE has been conducted in Blantyre, Malawi among inpatients and outpatients at QECH from July 1997 to June 2007, January 2008 to December 200937,38, and since January 201212,22, as previously described. Briefly, children <5 years of age who presented to QECH with acute gastroenteritis (AGE, defined as three or more loose stools in a 24-hour period for less than 14 days) and moderate to severe dehydration were enrolled, fecal samples were collected, and rotavirus testing was carried out using a sensitive and specific enzyme-linked immunosorbent assay (ELISA; Rotaclone®; Meridian Bioscience); the G- and P-types of rotavirus-positive samples were determined using reverse-transcriptase polymerase chain reaction (RT-PCR)39. We analyzed aggregate data on the number of rotavirus-positive and rotavirus-negative AGE cases in each week of the surveillance period through June 2022 for 1-month age categories <2 years of age and 1-year age categories for 2 to <5 years of age. The data collection protocols were approved by the National Health Sciences Research Committee, Lilongwe, Malawi (Protocol #867) and the Research Ethics Committee of the University of Liverpool, Liverpool, UK (000490) under the Diarrhoea Surveillance study; the modeling analysis was based on de-identified data and was deemed “not human subjects research” by the Yale University IRB (protocol ID 2000028875).
Sample collection was halted between April and early October 2020 due to the COVID-19 pandemic. Following the pandemic, healthcare seeking for diarrhea at QECH substantially declined before gradually increasing to pre-pandemic levels in 2022. To control for changes in healthcare seeking and reporting effort over time, we calculated the 2-year (105-week) moving average of the number of rotavirus-negative AGE cases in the <1 year, 1 to <2 year, and 2 to <5 years age groups; we then divided by the mean number of rotavirus-negative AGE cases for the entire surveillance period in each age group to estimate the relative reporting rate over time.
Vaccine coverage
Vaccination status was recorded on government-issued family-held records. To estimate vaccine coverage over time, we divided the number of age-eligible rotavirus-negative AGE cases who had received one or two doses of the RV1 vaccine by the total number of age-eligible rotavirus-negative AGE cases who presented to QECH in the 9-month (39-week) period centered on each week from October 28, 2012 (week of vaccine introduction) to June 2022. Uncertainty was quantified using 95% binomial confidence intervals.
The date of vaccination was available for a subset of individuals with data collected between January 2015 and June 2022. We used this information to calculate age at vaccination (in weeks) for both rotavirus-positive and rotavirus-negative AGE cases.
Mathematical models
To estimate the counterfactual number of RVGE cases that would be expected in each age group over time had the RV1 vaccine not been introduced, we used mathematical models that we previously developed and fitted to pre- and post-vaccination RVGE cases at QECH (Figs. S5, S6). Details of the modeling approach have been previously described14. Briefly, in the absence of vaccination, the model assumes that infants are born with maternal immunity, which wanes after a period of ~6 months. After each rotavirus infection, individuals are briefly immune to reinfection, then gain partial acquired immunity that reduces the severity and rate of subsequent infections; we assume the risk of moderate-to-severe RVGE is negligible following two natural infections. The model was parameterized based on data from birth cohort studies (see Table S3), then fitted to the 12 years of pre-vaccination data from QECH to estimate the mean transmission rate (as quantified by the basic reproductive number, R0), amplitude and timing of seasonality in transmission, and the proportion of moderate-to-severe RVGE cases in Blantyre that seek care at QECH and are tested (i.e., reporting fraction). To control for variation in reporting effort over time, we multiplied the reporting fraction by the relative reporting rate (described above). We initially fit the model via maximum a posterior estimation, then used a Markov chain Monte Carlo to obtain samples from the posterior distributions of model parameters (Table S3)14.
To model the effect of vaccination with RV1, we explored different assumptions about the probability of responding to each vaccine dose and the potential waning of vaccine-induced immunity. Models 1 and 2 assume that each vaccine dose provides immunity comparable to one natural infection among those who respond to the vaccine, i.e., partial immunity against reinfection and full protection against moderate-to-severe RVGE following two “successful” vaccine doses and/or natural infections. Model 1 assumes the proportions of infants who respond to the first and second dose are independent of one another (i.e., homogeneity in vaccine response), whereas Model 2 assumes that individuals who fail to respond to the first dose may be less likely to respond to subsequent doses (i.e., heterogeneity in vaccine response). The probability of responding to each dose was estimated based on seroconversion data from a vaccine trial conducted in Malawi10; uncertainty was characterized using beta distributions, as detailed previously (Table S4)14. Neither model was fitted to the post-vaccination data.
Models 3 and 4 assume each vaccine dose provides, among those who respond, temporary but complete immunity against rotavirus infection. Following the waning of vaccine-induced immunity, vaccinated infants return to their previous level of susceptibility, while those who respond to both vaccine doses move to the next vaccinated (and protected) compartment. Model 3 assumes homogeneity in vaccine response, whereas Model 4 assumes heterogeneity in vaccine response. The probability of responding to each vaccine dose and the rate of waning of vaccine-induced immunity were estimated by fitting to the post-vaccination data from QECH between October 2012 and August 2017 (Table S4)14.
Model validation
To validate model predictions for the impact of rotavirus vaccination in Malawi, we compared the predicted number of RVGE cases from the four models to the observed number of rotavirus-positive AGE cases at QECH. We considered both the total number of cases per week among children <5 years old as well as cases in each of the three age groups (<1 year, 1 to <2 years, and 2 to <5 years of age). First, we calculated the Spearman rank correlation coefficient and root mean square error (RMSE) between the model-predicted mean number of RVGE cases stratified by week and age group and the observed number of RVGE cases per week and age group for three time periods: the full 10-year time period from January 2012 to June 2022 (excluding the period from April to October 2020 with no surveillance); the in-sample validation period (January 2012–August 2017, previously used for fitting Models 3 and 4); and the out-of-sample validation period (September 2017–June 2022). Second, we calculated the proportion of weeks in which the 95% prediction interval for the model-predicted number of RVGE cases contained the observed number of RVGE cases. To generate the model predictions, we sampled 100 times from the joint posterior distributions of the pre- and post-vaccination model parameters. To account for observation error around the mean number of RVGE cases predicted for each week (comparable to the approach used for model fitting), we sampled 100 times from a Poisson distribution with rate parameter λw,a equal to the mean number of RVGE cases in week w and age group a for each of the 100 model simulations. The 95% prediction intervals were generated based on the 2.5 and 97.5 percentiles of the resulting 10,000 samples for each week (and within each age group) for the different models.
Overall effectiveness
Using the validated models, we then estimated the overall vaccine effectiveness for each year following the introduction of RV1 in 2012. For each of the models, we simulated both the predicted mean number of RVGE cases given the estimated vaccine coverage over time as well as the mean number of RVGE cases predicted with no vaccination (i.e., assuming vaccine coverage was 0%). All four models predicted the same number of RVGE cases in the absence of vaccination, as expected. Overall effectiveness (OE), defined as the reduction in disease incidence among both vaccinated and unvaccinated individuals in a vaccinated population compared to an unvaccinated population7, in year y and age group a was estimated as:
$$O_=1-\frac__}__,w,a}}$$
(1)
where Yw,a is the observed number of RVGE cases in week w (in year y) and age group a and Hnovacc,w,a is the model-predicted number of RVGE cases in week w and age group a with no vaccination.


留言 (0)