
記住我
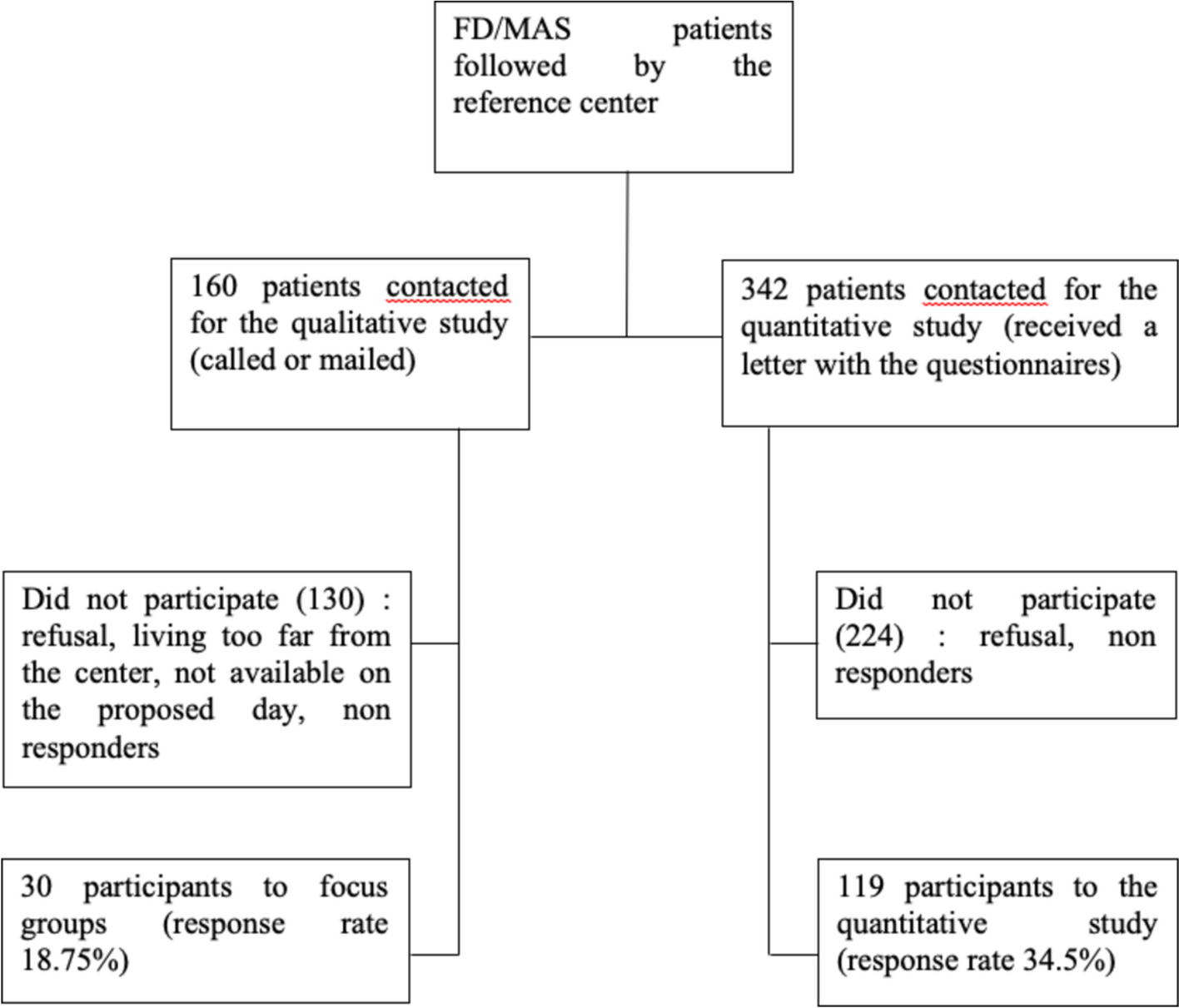
The literature search identified 62 publications after removal of duplicates (Fig. 1). After title screening of all 62 records, 42 articles were assessed as eligible for following abstract screening. The abstract screening resulted in 8 articles, all of which discussed transition in healthcare for OI [22, 23, 31,32,33,34,35,36]. In addition, the study separately included six recent articles extensively devoted to transition to other known chronic diseases based on a separate general search (not shown here) [37,38,39,40,41,42]. Summary of the articles included in the current review is given in Tables 1 and 2.
Factors Ensuring Success of OI Pediatrics to Adult Care TransitionAlthough different transition processes exist across various healthcare systems, the reviewed literature stratifies the experiences and guidelines of OI patients’ transition from pediatrics to adult care into several generalized key topics, which create critical elements to secure the success of the well-coordinated transition process. Interestingly, all available literature clearly emphasizes the need for improved guidelines for adult follow-up and care to improve transition outcomes. Challenges such as organizational changes, care discontinuation, and conflict of transition programs with ongoing research protocols must be carefully considered.
High Standards of OI Health Care and Transition RequirementsMaintaining health care during transition and the continuity of medical care from a multidisciplinary team after transition is crucial [32]. Thus, a single healthcare provider overseeing the patient’s care, ensuring a comprehensive view and integrating it into sound advice and policy, is essential. This lead healthcare provider keeps all disciplines informed and engaged in the specialized OI care, which is typically provided alongside their own specialties [32]. To ensure smooth care delivery, synergistic cooperation among the various involved disciplines and a clear allocation of tasks between clinicians and nurses is vital. The transition for individuals with OI is a complex process requiring a multidisciplinary approach to ensure high quality of care [31, 34]. Studies suggest that a structured, coordinated transition is crucial to avoid the fragmentation of services, which often occurs in adult care settings where the specialized networks of pediatric institutions may be lacking [31, 34]. The systemic nature of OI necessitates ongoing care from specialists like orthopedic surgeons, endocrinologists, audiologists, pulmonologists, cardiologists, ENT doctors, and rehabilitation professionals. However, adult care settings often fail to provide the same level of coordination, leading to disjointed treatments from various providers without a central coordinating role [22, 23].
The time taken for the consultation to transition of a patient from pediatric to adult care, undertaken by diverse medical specialists, is crucial [32]. Ensuring continuous, high-quality care fulfills the patient’s well-being and sense of security, particularly during the transition to adulthood [23]. Healthcare providers should address patients’ fears of pain and fractures, reassuring them of the “new” adult OI care team’s extensive experience with handling of OI patients, who need special management, fracture and pain treatment [35, 36]. This process demands a high level of expertise, and patience to earn the trust of an adapting OI patient. Recognizing fatigue during consultations is also vital for maintaining patient engagement in OI care. It is recommended that OI care can be provided in hospitals with specialized expertise, where the necessary organization and specialist knowledge are available. Ideally, these OI expertise hospitals should collaborate effectively with peripheral hospitals near the patient, sharing knowledge and remaining available for questions, with tailor-made check-ups. Providing an early and thorough explanation of the potentially different structure and organization of adult care facilities is important.
Individualized Approach of Transition ModelsVariability of healthcare systems, as well as variability of OI representation necessitates customized programs reflecting patient preferences. Personalized transition plans that take into account the unique needs and preferences of each patient are key to smooth transition [23]. These individual transition plans benefit from continuous evaluation and ongoing adjustments to ensure that they remain effective. Moreover, such customized individual plans are flexible enough to align with organizational activities, as transition programs have to be integrated within the healthcare center.
Shift in Prioritizing of Key Areas for OI Youth/Young Adults Well-BeingQualitative research of transition experiences, as well as previous questionnaires of adults with OI underline the shift of priorities in OI patient well-being and care after pediatric age, underlining changes in clinical impact of OI with aging [31, 43]. Focus from fractures and skeletal concerns changes to extraskeletal challenges, with highest impact on quality of everyday life affected by pain and fatigue, which is shared by (young) adult and adolescent OI patients [15]. According to adolescents, psychosocial components of the well-being also gain critical importance (e.g. accessibility, education, mental health, parental care and independence) [36]. The programs should address the broader impact of transition on young patients’ social lives and work readiness, ensuring adequate preparation for adult responsibilities.
Communication and AdvocacyA proactive patient and family involvement are an inherent component of the transition process. Young patients should be encouraged to take an active role in the transition process, promoting self-advocacy and coordination of care. At this moment partnership with parents is extremely important for a successful transition and fostering of a supportive environment [35]. Parents should not be fully excluded during and after the transition. However, protective strategies used by parents and their impact on OI youth undergoing transition, should be made clear with special attention to holistic approaches, which include understanding the experiences and perceptions of risk and vulnerability by both young people and their parents. This must be thoroughly discussed with the coordinating medical specialist, patient, and parents. Long-term parental assistance for this may be required.
Understanding frustration within all parties participating in the transition is equally important [34]. The young patient experiences challenges and frustrations related to the “unknown” status during the transition, and relies on mentorship and education to gain full independence. In addition, clinicians should be prepared and supported in managing the care of transitioning patients, who might need more guidance.
Transition Tools and Resources for OI YouthA number of transition tools were created by Canadian researchers to support OI transition.
(a) OI Transfer Summary Tool [22]: Provides a guidelines for a smooth transition, focusing on personalized care (available online and as pdf). It is an intriguing concept designed to ease the transition from pediatric to adult care. In hospitals with established electronic file systems, data can be seamlessly shared among healthcare providers, facilitating a straightforward transfer tool. However, in locations where such systems are not yet common, transferring the care history and various elements of the current pediatric care path becomes crucial.
(b) OI MyHealth Passport [33]: The tool enhances available organizational resources, aiding in the facilitation of care transitions, while ensuring gathering of patients’ data via self-management;
(c) Teens OI [36]: is an eHealth-based program to help youths manage their conditions and transition to adult care, empowering self-management for OI youth.
Transition to Adult Care Lessons from Other Chronic DiseasesAs more research has been conducted on transition in other chronic diseases, we reviewed the latest literature to determine if there are any important practices to consider in the context of transitioning within OI. From this literature the following structured common key preparatory steps emerged, aimed at preparing the adolescent for adult care: 1. Education, 2. Readiness, 3. Preparing, 4. Transition and 5 [35, 36, 43], Follow-up of the transition [38, 39, 44] (Fig. 2). In addition, peer support for the young adult also appeared to be of great importance outside the transition of care, as well as a responsible professional (doctor) who guides and monitors the transition. The latter may be the doctor himself or a representative of a healthcare organization. The medical knowledge transfer and the establishment/presence of a medical competent multidisciplinary team for adult care (care pathways) is also indispensable.
Fig. 2
Framework scheme encompassing five key steps (e.g. Education, Readiness, Preparing, Transition, Follow-up) of transition from pediatric to adult health OI care
Below we provide some examples.
Education is necessary to be ready for the transition. This has been highlighted in several articles on type 1 diabetes, juvenile arthritis and irritable bowel syndrome [38, 39, 44]. As an example of the latter, the readiness of Saudi adolescents with inflammatory bowel disease to transition from pediatric to adult care was assessed in a cross sectional study using the Transition Readiness Assessment Questionnaire (TRAQ). It turned out that the child’s level of education was the only independent variable that correlated with higher total scores. Patients over 15 years old had higher overall scores than younger patients [38].
Because the transition plays a major role in young people with type 1 diabetes (T1D), the American Academy of Pediatrics, American Academy of Family Physicians, and American College of Physicians jointly published the 2018 Clinical Report on the Guiding Principles of Healthcare Transition (HCT) [40]. This clinical report outlines six core elements of HCT in a structured process, which have been tested through partnership building using quality improvement methods. These have led to packages of the six core elements, available with resources and implementation guides. The six core elements include guide/policy (what to expect), tracking and monitoring (to ensure the adult is receiving the six core elements), readiness (of the adolescent), transition planning, transfer of care, transition confirmation (follow-up and feedback to the pediatric practice). However, they specifically target T1D [44].
In Juvenile arthritis (JIA) a patient-led study provided insight into the experience from the perspective of young people with JIA. They used a patient and Community Engaged Research (PaCER) approach and three focus groups, which showed the importance of readiness for the transfer of care, in developing self-advocacy skills, continuity of care (changing relationships, new responsibilities), need for support (social and mental health, beyond the transfer of care). Peer support was experienced as a very important overarching factor [39].
留言 (0)