The results of this large-scale population-based case–control study with real-world data suggest that in general, there is no association between previous use of traditional NSAIDs and the appearance of COVID-19 outcomes. Most of the NSAIDs evaluated are safe vis-à-vis the disease. It was, however, observed that diclofenac could be associated with a higher risk of progression to severe disease stages. Furthermore, according to our results, selective COX-2 inhibitors could reduce the risk of progression to severe diseases stages, though this association does not reach statistical significance.
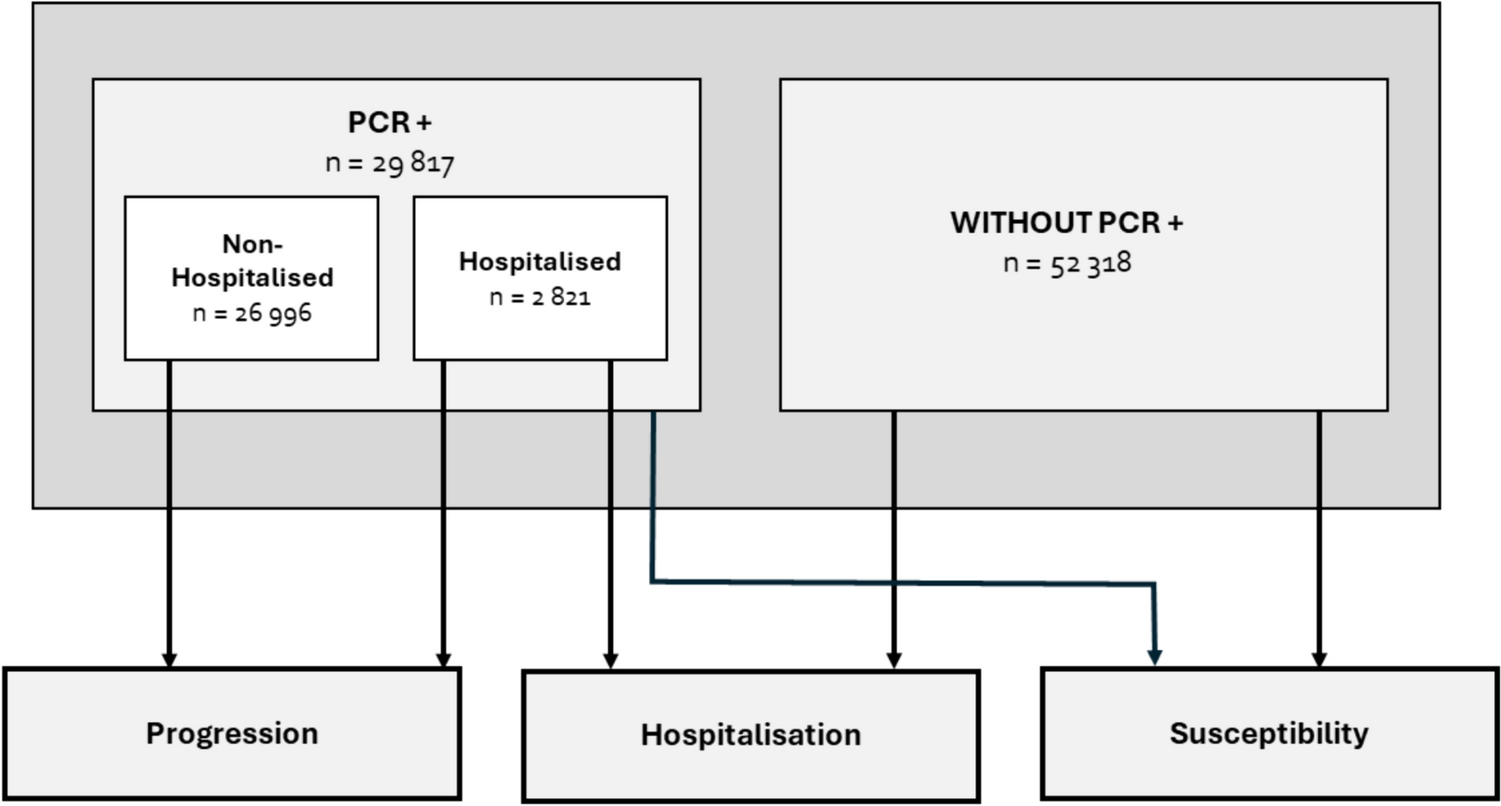
The design and size of our study sample enabled us to analyse the effect of NSAIDs by active ingredient and type (traditional NSAIDs and selective COX-2 inhibitors) on a number of COVID-19 outcomes, such as susceptibility, PCR + patient progression, and hospitalisation.
With respect to traditional NSAIDs (dexketoprofen, ibuprofen, naproxen, meloxicam, aceclofenac, lornoxicam, and metamizole), no association was found between their use in the last month and the outcomes analysed, despite the high statistical power of our study (n = 82 135). In contrast, diclofenac showed a significant increase in risk of progression to severe stages of the disease (aOR = 1.80; 95% CI 1.12–2.88). Although we cannot rule out that this may be a chance finding, our result is nonetheless in line with a previous study which identified a higher risk of cardiovascular and coronary events in COVID-19 patients who used diclofenac (Campbell et al. 2022a).
The outcomes of selective COX-2 inhibitors are more noteworthy, since they suggest a possible decrease in risk of disease progression, close to statistical significance (aOR = 0.70; 95% CI = 0.47–1.04, p < 0.08). These observations are in line with the previous studies, which suggest that selective COX-2 inhibitors could be useful in SARS-CoV-2 infection for relieving COVID-19-related symptomatology (Ong et al. 2020; Hong et al. 2020; Ghaznavi et al. 2022; Consolaro et al. 2022).
The biological plausibility of this possible association is based on a number of previously proposed mechanisms. First, COX-2 inhibition could modulate the excessive inflammatory response observed in severe cases of COVID-19, decreasing the levels of proinflammatory cytokines, such as TNF-α, G-CSF and IL-6, and preventing progression to more severe disease stages (Baghaki et al. 2020). Furthermore, it has been shown that COX-2 inhibitors possess antifibrotic effects (Fabbrini et al. 2009; Tseng et al. 2019), which could be beneficial for preventing or reducing pulmonary fibrosis associated with COVID-19. Similarly, it has been suggested that these drugs could modulate antiviral immunity without compromising the general immune response, unlike non-selective NSAIDs, which on inhibiting both COX-1 and COX-2 could weaken the antiviral response (Baghaki et al. 2020). This capacity of selective COX-2 inhibitors to maintain an appropriate balance between immune response and excessive inflammation could be fundamental in the management of COVID-19 patients.
The biological mechanisms suggested, along with the similarity in the odds ratios observed in our study between the selective COX-2 inhibitors most prescribed in Spain (celecoxib and etoricoxib), support the idea that the reduction in the risk of disease progression could be a class effect. That said, however, more studies are needed, preferably randomised clinical trials (RCT) such as those that are under way (NCT05077332, NCT04488081), to confirm these findings and ascertain the efficacy and safety of selective COX-2 inhibitors in patients with COVID-19.
It would be relevant to continue studying the antiviral potential of selective COX-2 inhibitors, such as celecoxib and etoricoxib. Previous studies on preclinical models have stressed the antiviral activity of these compounds against different viruses, such as herpes simplex, hepatitis C, dengue, or zika. Furthermore, they have been identified as one of the few treatments available, with RCT-based evidence which shows that they reduce mortality in severe influenza. The development of this line of research could make for a better understanding of the antiviral activity of selective COX-2 inhibitors and their usefulness in different viral infections.
Clinical and public health implications
If the results of ongoing RCT of selective COX-2 inhibitors confirm the trend observed in our study toward a reduction in risk of disease progression, the use of these drugs in the management of COVID-19 could have a dual purpose. Apart from relief of symptoms, such as fever, pain, and inflammation, they could influence disease progression, reducing the risk of severe complications and the need for hospitalisation in infected patients.
It is important to stress that the results relating to disease progression are currently of great relevance. If previous use of selective COX-2 inhibitors is associated with a decrease in disease progression, it is plausible that their use during the symptomatic stage could likewise influence this. In turn, this potential effect could also decrease the risk of hospitalisation, an outcome of great public health interest.
With respect to the impact of the use of NSAIDs (including traditional NSAIDs and selective COX-2 inhibitors) during the symptomatic stage, we decided not to perform these analyses due to a possible bias of inverse causality. This phenomenon refers to the possibility of disease severity influencing the use of NSAIDs, rather than the use of NSAIDs influencing disease severity. This bias cannot be adequately controlled for by the design of our study. It is, however, important to consider that patients could continue taking these drugs during the symptomatic stage due to previous or recent prescriptions in the days preceding detection of the virus. Our results suggest that use of NSAIDs neither negatively affects nor protects patients during this stage, and that the use of selective COX-2 inhibitors could be associated with a reduction in risk.
Strengths and limitations
The main strengths of our study are its use of population data and large sample size, which made it possible to adjust the results for a wide range of clinical and socio-demographic variables. This enabled us to accurately estimate the possible association between use in the last month of different NSAIDs and susceptibility to and prognosis of COVID-19 (progression to severe stages and hospitalisation). Furthermore, the measure of exposure to drugs was based on dispensing data, something that reduces the risk of misclassification of the variable of exposure, as compared to many other studies which use prescription-based data-sources. It should be stressed that here in Spain, most NSAIDs cannot be dispensed without a medical prescription, so that dispensing provides a good estimate of their use.
Our study also has some limitations. First, the fact of its being an observational study with secondary databases means that there is the possibility of residual confounding due to unmeasured or misclassified factors, such as the degree of severity of the main comorbidities associated with greater COVID-19 severity. Moreover, the lack of matching in the susceptibility and progression substudies could be considered a further limitation, though the validity of the study is not really affected, since the absence of matching only decreases efficacy and does not increase the risk of biases (Rothman et al. 2008; Rose and Laan 2009). It should also be borne in mind that the data available for this study pertain to 2020, when the predominant SARS-CoV-2 variants in this country were derived from clade 19B (Díez-Fuertes et al. 2021), though we have no reason to believe that the effect of the drugs studied against COVID-19 could be influenced by the presence of the dominant variant. Finally, it should be noted that our study lacks a dose–response analysis of exposure to the drug and the trend in the outcomes, which limits a complete understanding of the relationship between the dose of the drugs and their effects on development of the disease.




留言 (0)