
記住我


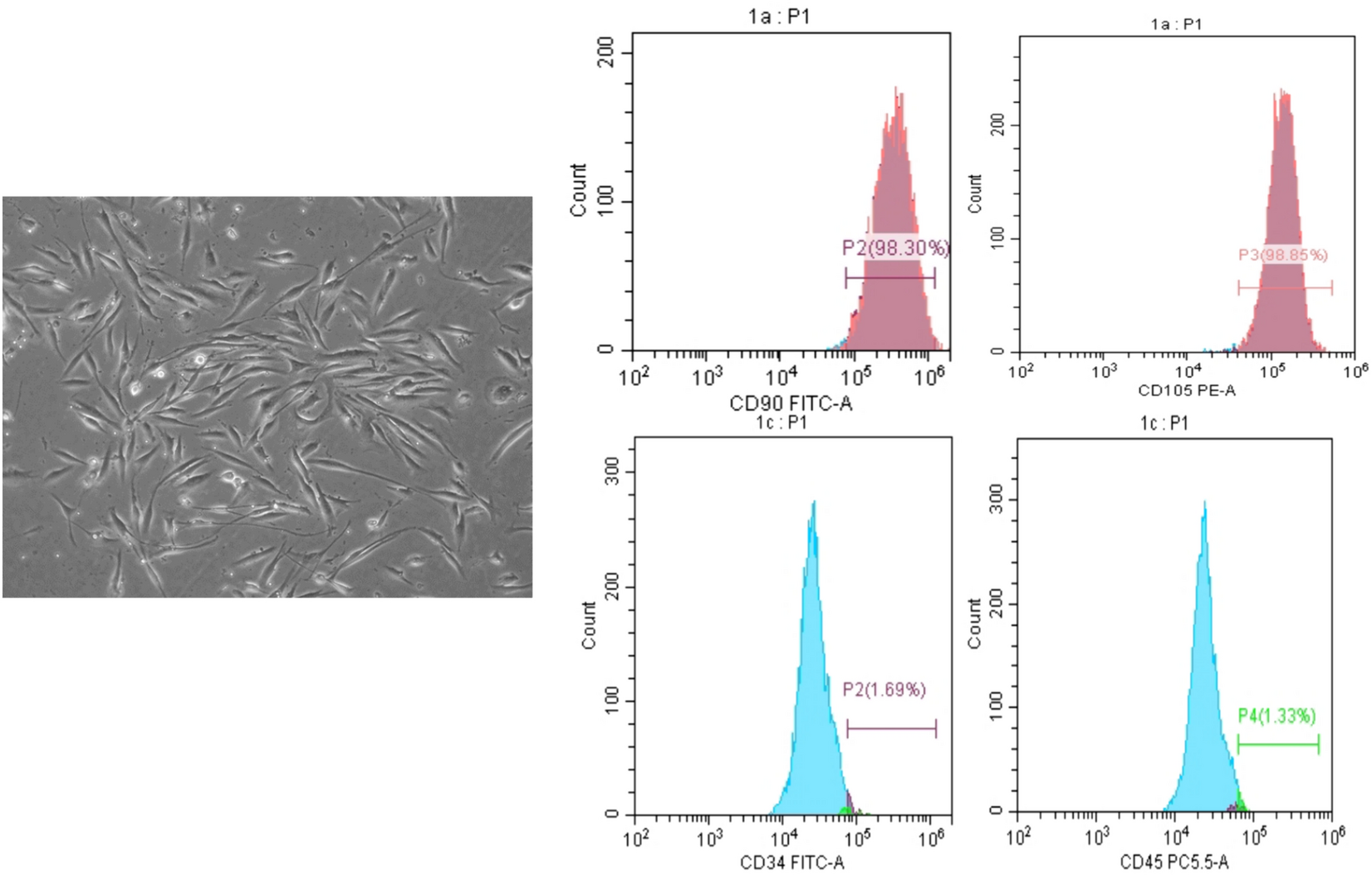

A few days after culture, microscopic observation of the isolated cells revealed stellate-shaped fibroblast-like cells that were adherent to the culture plate and demonstrated signs of proliferation. Moreover, flow cytometric analysis confirmed that the isolated dental pulp stem cells (DPSCs) were mesenchymal stem cells (Fig. 1a). The isolated cells exhibited positive expression of specific mesenchymal stem cell markers, namely, CD90 and CD105, while the expression of the hematopoietic markers CD34 and CD45 was negative (Fig. 1b).
Fig.1
Morphological observation and flow cytometric characterization of isolated DPSCs. The cells exhibited a fibroblast-like appearance. The cells exhibited positive expression of CD90 (98.3%) and CD105 (98.8%) and negative expression of CD34 (1.69 Images of colon tissue 15 days %) and CD45 (1.33%)
(2) Combinatorial intervention with DPSCs and sulfasalazine mitigated the macroscopic appearance of the colon in ulcerative colitis-challenged ratsThe potential impact of coadministering DPSCs with sulfasalazine on mitigating inflammatory symptoms in ulcerative colitis was initially assessed by macroscopically observing the length of the colon in an ulcerative colitis rat model after 15 days of induction (Fig. 2a). The macroscopic appearance of the colon was significantly greater in the DPSC-treated rats than in the sulfasalazine-treated rats. A significant difference between acetic acid (AC. a) and acetic acid + sulfasalazine + DPSC, and acetic acid (AC. a) + sulfasalazine and acetic acid (AC. a) + DPSCs was evident. Notably, compared with those in all the other groups, the colon length in the DPSCs and sulfasalazine-treated rats was significantly greater (Fig. 2b).
Fig. 2
after ulcerative colitis induction (left): (a) control, (b) 3% acetic acid, (c) DPSCs, (d) sulfasalazine 30, and (d) DPSCs + sulfasalazine 30. Effect of different treatments on colon length in an induced ulcerative colitis rat model (right). a: Significant difference between the control and (AC treatments. a) group. b: Significant difference between (AC. a) and (AC. a) + DPSCs. c: Significant difference between (ACs. a) and (AC. a) + sulfasalazine. d: Significant difference between (AC. a) and (AC. a) + sulfasalazine + DPSCs. e: Significant difference between (ACs. a) + DPSCs and (AC. a) + sulfasalazine + DPSCs. f: Significant difference between (ACs. a) + sulfasalazine and (AC. a) + DPSCs. (AC. a): acetic acid, DP. MSCs: dental pulp mesenchymal stem cells. Significant difference at P < 0.05
(3) Combined administration of DPSCs and sulfasalazine attenuated edema of colon tissue in ulcerative colitis-challenged ratsThe ratio of colon weight to length was investigated as a marker of ulcerative colitis-associated colonic edema. The edema marker demonstrated a significant increase in rats treated with acetic acid- (AC. a) induced ulcerative colitis compared to that in control counterparts. However, compared with that in the acetic acid- (AC. a) administered group, sulfasalazine administration alone significantly decreased edema markers in relation to acetic acid- (AC. a) administered group. Moreover, compared with acetic acid (AC. a) and sulfasalazine-treated groups. These results suggested that DPSC administration alone or in combination with sulfasalazine significantly attenuated colonic edema in acetic acid-induced ulcerative colitis in rats (Fig. 3).
Fig. 3
Effect of different treatments on edema marker of colon tissue of induced ulcerative colitis in rats. a: Significant difference between control and (AC. a) group. b: Significant difference between (AC. a) and (AC. a) + DPSCs. c: Significant difference between (AC. a) and (AC. a) + sulfasalazine. d: Significant difference between (AC. a) and (AC. a) + sulfasalazine + DPSCs. e: Significant difference between (AC. a) + DPSCs and (AC. a) + sulfasalazine + DPSCs. f: Significant difference between (AC. a) + sulfasalazine and (AC. a) + DPSCs. (AC. a) acetic acid, DP. MSCs Dental pulp mesenchymal stem cells. Significant difference at P < 0.05
(4) DPSCs and sulfasalazine regulated reactive oxygen species (ROS) and xanthine oxidase (XOD) activity in induced ulcerative colitis-challenged ratsAny disruption in the equilibrium between antioxidation and oxidation is regarded as critical for determining the severity of ulcerative colitis. Initially, the level of ROS was assessed as an indicator of oxidative stress in the colon in all the groups under investigation (Fig. 4a). The level of ROS was markedly elevated in the groups with ulcerative colitis induced by acetic acid (AC. a) compared to the control group. Nevertheless, the administration of either DPSCs or sulfasalazine, either individually or in combination, led to a significant decrease in the level of reactive oxygen species (ROS) in contrast to that in the ulcerative colitis group induced by acetic acid (AC. a). The most significant suppression of ROS was observed when DPSCs were treated with sulfasalazine.. The antioxidant activity was also examined in the colonic tissue of all the groups under study. The administration of acetic acid (AC. a) treatment led to significant inhibition of XOD activity compared with that in the controls (Fig. 4b). Notably, the administration of DPSCs and sulfasalazine, either separately or in combination, significantly promoted XOD activity, contrary to that in the ulcerative colitis group induced by acetic acid (AC. a). The most prominent and pronounced increase in XOD was observed in the colons of rats with induced colitis when sulfasalazine and DPSCs were administered in combination.
Fig. 4
(a) Effect of different treatments on reactive oxygen species (ROS) of colon tissue of induced ulcerative colitis in rats. (b) Effect of different treatments on xanthine oxidase (XOD) activity of colon tissue of induced ulcerative colitis in rats. a: Significant difference between control and (AC .a) group. b: Significant difference between (AC. a) and (AC. a) + DPSCs. c: Significant difference between (AC .a) and (AC. a) + sulfasalazine. d: Significant difference between (AC. a) and (AC. a )+ sulfasalazine + DPSCs. e: Significant difference between (AC. a) + DPSCs and (AC. a) + sulfasalazine + DPSCs. f: Significant difference between (AC. a) + sulphasalazine and (AC. a) + DPSCs. Significant difference at P < 0.05. (Ac. a) acetic acid, DP. MSCs dental pulp mesenchymal stem cells
(5) DPSCs and sulfasalazine administration ameliorated histological alterations in colon tissues from induced ulcerative colitis ratsThe control groups exhibited the typical histological characteristics of the mucosa, muscularis layers, and submucosa in the colon (Fig. 5 a). The acetic acid (AC. a) group displayed patchy loss of the normal surface epithelium, distortion of the normal crypt architecture, degeneration of mucosal cells, and inflammatory infiltration in the mucosa and submucosa in the presence of hemorrhage (Fig. 5b). The group treated with acetic acid (AC. a) + DPSCs showed a normal histological structure with an intact mucosal epithelium and muscularis layers with only slight inflammatory infiltration of the mucosa and submucosa (Fig. 5c). The group treated with a combination of acetic acid (AC. a) and sulfasalazine exhibited a modest improvement, accompanied by a slight loss of a few surface columnar epithelial cells. Additionally, slight inflammatory infiltration was observed in both the mucosa and submucosa (Fig. 5d). In the group treated with acetic acid (AC. a) + sulfasalazine + DPSCs, the histological structure was noticeably improved, the mucosal epithelium was intact, and only mild inflammatory infiltration in the mucosa and submucosa was observed with slight hemorrhage (Fig. 5e).
Fig. 5
Representative photomicrographs of H&E-stained colon sections. (a) Photomicrograph of a section in the colon from the control group showing normal structure of mucosa with an intact epithelial surface (M), muscularis layers (Mm), and submucosa (Sm). (b) Groups treated with acetic acid demonstrating patchy loss of normal surface epithelium (arrowhead), distortion of normal crypts architecture, degenerated cells of mucosa (M), inflammatory infiltration in the mucosa (arrow) and submucosa (Sm) with the presence of hemorrhage (star). (b) Groups treated with acetic acid and hDPSCs showing normal histological structure with intact mucosal epithelium (M), muscularis layers (Mm) only slight inflammatory infiltration mucosa (yellow arrow) and submucosa (Sm). (c) Groups treated with acetic acid and sulfasalazine illustrating moderate improvement with minor loss of some surface columnar epithelial cells (arrowhead), there was mild inflammatory infiltration in the mucosa (arrow) and submucosa (Sm). (d) Groups treated with acetic acid and (sulfasalazine + hDPSCs) demonstrating noticeable improvement of the histological structure with intact mucosal epithelium (M), only a mild inflammatory infiltration in the mucosa (arrow), submucosa (Sm) and slight hemorrhage (star). (a) Control, (b) (AC. a), (c) AC. a + DPSCs, (d) AC. a + sulfasalazine, (e) (AC. a )+ sulfasalazine + DPSCs. Mucosa (M), submucosa (Sm), muscularis layers (Mm), slight hemorrhage (star)
(6) Administration of DPSCs and sulfasalazine downregulated the expression of IL-1β and NFκB-p65 in ulcerative colitis-challenged ratsThe expression of IL-1β and NFκB-p65 was investigated immunohistochemically to provide further insights into the inflammatory status of the colon tissue and the potential effectiveness of DPSC and sulfasalazine administration in modulating the inflammatory response. The expression of both IL-1β and NF-κB-p65 in the colon tissues of rats significantly increased in comparison to that of control rats when acetic acid (AC. a) was administered to induce ulcerative colitis in rats. Figures 6and 7 depict the percentage and intensity of positive cells stained for IL-1β and NF-κB-p65, respectively. Normal colon mucosa in the control group exhibited weak IL-1β staining on the cell membranes, which illustrated a staining intensity nearly equivalent to that of the background staining (Fig. 6a). Conversely, the acetic acid (AC. a) group cells exhibited a high percentage of IL-1β-positive cells, which were primarily localized in the nuclei, in comparison to the control group (Fig. 6b). Therefore, IL-1β expression greatly increased in response to the acetic acid (AC. a) group, whereas it markedly decreased in the groups that received DPSCs and sulfasalazine alone (Fig. 6c, d). Nevertheless, the expression levels of IL-1β were significantly lower in DPSCs administered in combination with sulfasalazine than in those in all the other groups (Fig. 6e). However, neither DPSCs nor sulfasalazine independently affected IL-1β expression compared to the control (Fig. 6f). NFκB-p65 was weakly expressed at the cell membrane of the colon mucosa in the control group (Fig. 7a). The acetic acid (AC. a) group demonstrated intense staining of the nuclei with a significantly increased number of positive cells (Fig. 7b). The DPSC- and sulfasalazine-treated groups showed significantly lower staining intensity and percentage of positive cells than did the acetic acid (AC. a) group (Fig. 7c). Remarkably, the combination of DPSCs and sulfasalazine significantly diminished both the staining intensity and percentage of cells positive for NF-κB-p65 compared to those of all the other groups (Fig. 7f). Like the findings observed with IL-1β staining, neither DPSCs nor sulfasalazine separately affected the expression of NF-κB-p65 compared to that in the control group (Fig. 7d, e). Taken together, these results demonstrated that the combined administration of DPSCs and sulfasalazine alleviated the expression of inflammatory markers, such as IL-1β and NF-κB-p65, indicating the potent role of their combined administration in the recovery of the inflammatory response induced by UC.
Fig.6
Immunohistochemical staining against IL-1β in colonic sections of different treatment groups. (a) Photomicrograph showing negative reaction for IL-1β in intestinal mucosa in the control group. (b) Groups treated with acetic acid showing strong positive reaction for IL1β in cytoplasm of intestinal glands (arrows). (c) Groups treated with acetic acid and hDPSCs showing negative reaction for IL-1β in the intestinal mucosa. (d) Groups treated with acetic acid and sulfasalazine illustrating strong positive reaction for IL1β in the cytoplasm of inflammatory cells in the intestinal mucosa (arrows). (e) Groups treated with acetic acid and (sulfasalazine + hDPSCs) showing negative reaction for IL-1β in the intestinal mucosa. (f) Expression of IL-1β in the studied groups. Data presented as mean and standard deviation. (a) Control. (b) (AC. a). (c) (AC. a) + DPSCs. (d) (AC. )a + sulfasalazine. (e) (AC. a) + sulfasalazine + DPSCs. Significant difference at P < 0.05
Fig. 7
Immunohistochemical staining against NFκB-p65 in colonic sections of different treatment groups. (a) Photomicrograph showing negative reaction for NFKB-p65 in intestinal mucosa of the control group. (b) Groups treated with acetic acid showing strong positive reaction for NFKB-p65 in nuclei and cytoplasm of the intestinal epithelium (yellow arrow), in nuclei of inflammatory cells (red arrow) between intestinal villi (c) groups treated with acetic acid and hDPSCs showing positive reaction for NFKB-p65 in the nuclei of intestinal epithelium (red arrow). (d) Groups treated with acetic acid and sulfasalazine showing strong positive reaction for NFKB-p65 in the cytoplasm of intestinal villi (yellow arrow) and nuclei of inflammatory cells between villi (red arrow). (e) Groups treated with acetic acid and (sulfasalazine + hDPSCs) demonstrating negative reaction for NFKB-p65 in the intestinal mucosa. (f) Expression of NFKB-p65 in the studied groups. Data presented as mean and standard deviation. (a) Control. (b) (AC. a). (c) (AC. a) + DPSCs. (d) (AC. a) + sulfasalazine. (e) (AC. a) + sulfasalazine + DPSCs. Significant difference at P < 0.05
(7) Administration of DPSCs and sulfasalazine suppressed the levels of proinflammatory cytokines in the colons of ulcerative colitis-challenged ratsTo investigate the improvement in the immune response that could have resulted from the administration of DPSCs alone or in combination with sulfasalazine, the levels of proinflammatory cytokines were analyzed in the colon tissues of all the subjects studied (Fig.8). Enzyme-linked immunosorbent assays (ELISA) were utilized to assess the levels of TNF-α (Fig.8a), NF-κB-p65 (Fig.8b), and TLR-4 (Fig.8c) in the colon. Comparing acetic acid (AC. a) with those in the control group, the levels of TNF-α, NF-κB-p65, and TLR-4 in the colon were significantly greater. Although the administration of DPSCs or sulfasalazine alone resulted in a significant reduction in the levels of the tested proinflammatory cytokines in the colon, the combination of both DPSCs and sulfasalazine significantly resulted in an even greater reduction in the levels of those cytokines in the colon than the acetic acid (AC. a) group.
Fig. 8
Effect of different treatments on the levels of proinflammatory cytokines according to ELISA. (a) TNF-α (pg/mg), (b) NFκB-p65 (ng/mg protein) and (c) TLR-4 (ng/mg protein). a: Significant difference between the control and (AC. a) group; b: significant difference between (AC. a) and (AC. a) + DPSCs; c: significant difference between (AC. a) and (AC. a) + sulfasalazine; d: significant difference between (AC. a) and (AC. a) + sulfasalazine + DPSCs; f: significant difference between (AC. a) + sulfasalazine and (AC. a) + DPSCs. A P value < 0.05 indicated a significant difference. Ac. a acetic acid, DP. MSCs dental pulp mesenchymal stem cells.
(8) Administration of DPSCs and sulfasalazine downregulated the expression of the MyD88, NFκB and TLR-4 genes in the colon tissues of ulcerative colitis-challenged rats.To validate the anti-inflammatory properties of DPSCs and sulfasalazine in inhibiting the progression of UC, gene expression analyses were conducted for MyD88, NF-κB and TLR-4 (Fig. 9). The expression levels of the MyD88, NF-κB and TLR-4 genes in rat colon tissues were significantly upregulated in the acetic acid (AC. a) group in comparison to the control counterparts. In contrast, the expression levels of the MyD88, NF-κB and TLR-4 genes in both the DPSC-treated group and the sulfasalazine-treated group were significantly lower than those in the acetic acid (AC. a) group. The combined administration of DPSCs and sulfasalazine significantly downregulated the MyD88 (Fig. 9a), NF-κB (Fig. 9b) and TLR-4 (Fig. 9c) gene expression levels compared with those in the control group.
Fig. 9
qRT-PCR of MyD88, NF-κB and TLR4 markers in colon tissue of ulcerative colitis-challenged rats. (a) Expression level of MyD88 gene. (b) Expression level of NF-κB gene (c) Expression level of TLR-4 gene. a: Significant difference between the control and (AC. a) group, b: Significant difference between (AC. a) and (AC. a) + DPSCs. c: Significant difference between (AC. a) and (AC. a) + sulfasalazine. d: Significant difference between (AC. a) and (AC. a) + sulfasalazine + DPSCs. e: Significant difference between (AC. a) + DPSCs and (AC. a) + sulfasalazine + DPSCs. f: Significant difference between (AC. a) + sulfasalazine and (AC. a) + DPSCs. Significant difference at P < 0.05. Ac. a acetic acid, DP. MSCs dental pulp mesenchymal stem cells
Ulcerative colitis is a chronic inflammatory disease of the intestine that unfortunately lacks a definitive therapeutic approach. During the initial phases, many patients are typically prescribed aminosalicylates, specifically sulfasalazine, which is the most frequently recommended anti-inflammatory medication. However, patients using sulfasalazine frequently experience severe side effects, including nausea, vomiting, and hemolysis. Thus, to mitigate these adverse effects, it is crucial to adopt innovative therapeutic strategies. One of these strategies is to integrate stem cells into the treatment regimen through combination therapy.
The purpose of the present research was to assess the efficacy of combining DPSCs with sulfasalazine in acetic acid-induced ulcerative colitis in rats. The proposed therapeutic effect of combining dental pulp stem cells (DPSCs) and sulfasalazine arises from the synergistic integration of the advantages offered by both approaches. DPSCs possess a potent immunomodulatory effect, which results in a reduction of autoimmune inflammation and facilitates the healing of the intestinal mucosa. The anti-inflammatory action of sulfasalazine enhances this effect. Consequently, this approach shall extend the length of time during which the disease is inactive, reduces the likelihood of recurring episodes, and lessens the frequency of being admitted to the hospital.
It has been previously documented that acetic acid administration in rats results in an ulcerative colitis model similar to that in humans (Fabia et al. 1992; Low et al. 2013; El-Akabawy and El-Sherif 2019). It causes damage to the distilled colon portion and results in nontransmural inflammation. Moreover, acetic acid also provokes necrotic changes in both the mucosal and submucosal layers, including neutrophil infiltration and submucosal ulceration (Nakhai et al. 2007).
The use of DPSCs in the present study demonstrated the characteristic morphological features of mesenchymal stem cells, including a fibroblast-like appearance and adherence to growth plates. DPSCs were also characterized by flow cytometry, and their mesenchymal stem cell identity was confirmed through the positive expression of CD90 and CD105 and negative expression of CD34 and CD45. DPSCs were chosen for their ease of accessibility and for their remarkable immunomodulatory properties (Gronthos et al. 2002; Huang et al. 2009b, a; Wada et al. 2013; El-Moataz et al. 2018). In this context, previous studies have reported that MSCs exert regenerative therapeutic effects on induced colitis models by orchestrating and reducing immune cell infiltration into the colon (Zhang et al. 2009). In the present study, compared with those in the other groups, all the investigated macroscopic and microscopic signs of inflammation were markedly improved after the combined administration of sulfasalazine and DPSCs. DPSC transplantation significantly attenuated colonic edema, likely due to the anti-inflammatory characteristics of DPSCs. This effect was further enhanced when DPSCs were combined with sulfasalazine, suggesting that the combination of these agents augmented the anti-inflammatory effect of sulfasalazine, leading to this significant change. Our results align with those of Yousefi-Ahmadipour et al. (2019), who investigated the role of adipose-derived stem cells in combination with sulfasalazine in a rat model of inflammatory bowel disease (Yousefi-Ahmadipour et al. 2019). The dosage utilized in our study was estimated based on prior research conducted on comparable animal models (Yousefi-Ahmadipour et al. 2019). Prior studies have determined that mesenchymal stem cells obtained from bone marrow showed no signs of toxicity at a dosage of 252 × 106 cells/kg b.w. in rats. Thapaswini et al. (2022) reported that DPSCs showed no adverse reactions at concentrations of up to 10 million cells per mL (Thapaswini et al. 2022).
Our histological findings further confirmed the macroscopic results obtained in the validation of the ulcerative colitis model and in the establishment of the healing effect of DPSCs alone or in combination with sulfasalazine. Histopathological examination of colon tissue from acetic acid-induced rats revealed patchy loss of normal surface epithelium, distortion of the normal crypt architecture, degeneration of mucosal cells, and inflammatory infiltration in the mucosa and submucosa in the presence of hemorrhage. This occurrence can be attributed to the impact of acetic acid on the induction of colonic damage, subsequently resulting in epithelial mucosal destruction followed by inflammation. Acetic acid causes inflammation mainly through the infiltration of its soluble protonated form into the epithelium, which in turn causes intracellular acidification, leading to severe destruction of the epithelial layer (Nakhai et al. 2007; Soliman et al. 2016). Sections of the acetic acid- and sulfasalazine-treated group illustrated adequate improvement with minimal reduction of some surface columnar epithelial cells; there was mild inflammatory infiltration in the mucosa and submucosa. These results are in line with the results of previous studies (El-Akabawy and El-Sherif 2019; Yousefi-Ahmadipour et al. 2019). Notably, after DPSC therapy, normal histological structures with intact mucosal epithelium and muscularis layers and only slight inflammatory infiltration in the mucosa and submucosa were observed. These results resemble those of Yousefi-Ahmadipour et al. and could be explained by the possibility that the engrafted DPSCs differentiated into colonic interstitial lineage cells (Yousefi-Ahmadipour et al. 2019). However, the combined administration of DPSCs and sulfasalazine resulted in a noticeable improvement in histological structure, with an intact mucosal epithelium and mild inflammatory infiltration in the mucosa and submucosa, with slight hemorrhage.
To further elaborate the potential therapeutic role of DPSCs in the treatment of ulcerative colitis, oxidative stress markers (ROS and XOD) were investigated. Oxidative stress is a crucial factor in the pathogenesis of ulcerative colitis progression. The ROS concentration reflects the degree of oxidative stress associated with inflammation due to the occurrence of a certain amount of damage. On the other hand, XOD functions as an antioxidant that degrades ROS and prevents cells from undergoing peroxidation. The release of inflammatory cytokines disrupts the equilibrium between antioxidation and oxidation, which triggers the inflammatory response. This in turn causes damage to intestinal cells and destruction of the mucosal barrier (Wang et al. 2019; Benhar 2020). In our study, the administration of either DPSCs or sulfasalazine, either individually or in combination, significantly reduced ROS levels and significantly increased XOD activity. The most prominent and significant improvement was observed when sulfasalazine and DPSCs were administered in combination. The inhibitory effect of DPSCs on oxidative stress has been documented by (Al-Serwi et al. 2021) in a rat model of diabetes mellitus. Mesenchymal stem cells (MSCs) have both enzymatic and nonenzymatic biological mechanisms that help in neutralizing ROS (Hernández-Monjaraz et al. 2020). Moreover, DPSCs have been found to possess antioxidative characteristics (Song et al. 2015), supporting the proposed antioxidant abilities of MSCs (Silva et al. 2003).
Regarding sulfasalazine, Joshi et al. (2005) studied the reactions of sulfasalazine and its metabolites with various oxidizing and reducing free radicals to understand the mechanistic aspects of sulfasalazine action against free radicals produced during inflammation. Those investigators emphasized the ability of sulfasalazine and its metabolites to scavenge various primary and secondary free radicals. In addition, a recent study by Liu et al. (2020) revealed that sulfasalazine attenuates acetic acid-induced colitis in rats via the inhibition of oxidative stress (Liu et al. 2020). Furthermore, the antioxidative mechanism of sulfasalazine as a major path of pharmacological action against colitis has been confirmed by the latest study of Abdelmonaem et al. (2021), who found that sulfasalazine administration in colitis-bearing rats significantly reduces the colonic level of malondialdehyde, an indicator of oxidative stress, and normalizes total antioxidant capacity and superoxide dismutase activity, which are indices of the antioxidant defense system (Abdelmonaem et al. 2021).
As expected, acetic acid administration significantly elevated the levels of all the studied proinflammatory cytokines (TNF-α, NFκB-P65, and TLR-4) in the colon. Although the administration of DPSCs or sulfasalazine alone led to a significant reduction in the levels of the tested proinflammatory cytokines in the colon, the combination of both DPSCs and sulfasalazine drastically decreased the levels of those cytokines in the colon. Consequently, we proposed that the combination of DPSCs and sulfasalazine ameliorates UC through the inhibition of both inflammatory and oxidative stress processes.
Furthermore, the immunohistochemical results of the present study demonstrated that the combined administration of DPSCs and sulfasalazine attenuated NFκB-p65 and IL-1β expression. Interleukin-1β (IL-1β) is a major cytokine associated with the activation of proinflammatory signaling pathways and monocytes in peripheral tissues and has been described as an important mediator of the onset of ulcerative colitis-related inflammation (Liso et al. 2022). On the other hand, NF-κB was reported to play a crucial role in the pathogenesis of ulcerative colitis, as indicated by the upregulation of the expression of several inflammatory markers (Li et al. 2005). Interestingly, neither DPSCs nor sulfasalazine were able to reduce IL-1β and NFκB-p65 expression on their own. These findings provide further evidence for the hypothesis that combined therapy involving both DPSCs and sulfasalazine is fundamental for optimizing the efficacy of both agents, which will in turn contribute to more beneficial clinical results.
Finally, we further investigated the molecular role of both DPSCs and sulfasalazine through analyzing the gene expression levels of MyD88, NF-κB and TLR4 in an ulcerative colitis-induced rat model. MyD88 plays a pivotal role in modulating the immune response and inflammatory processes associated with colitis (Saikh 2021). It has been reported that NF-KB activation in patients with inflammatory bowel disease promotes mucosal inflammation by enhancing the expression of numerous proinflammatory genes (Atreya et al. 2008; Mohammad Jafari et al. 2021). Like the pattern delineated in the results previously outlined in the present study, the combined administration of DPSCs and sulfasalazine significantly downregulated MyD88, NF-κB and TLR4 gene expression. The specific mechanism underlying the anti-inflammatory and immunomodulatory activities of DPSCs is complicated. DPSCs likely modulate immune cells via inflammatory immune-related signaling pathways (Li et al.
留言 (0)