2.1 BIO-RESORT trial design, procedures and follow-up
This health economic evaluation was performed using comprehensive clinical outcome data of the randomised BIO-RESORT trial (NCT01674803). The study design and details of BIO-RESORT have been reported previously [6]. In brief, the BIO-RESORT trial is a large-scale, investigator-initiated, randomised study that assessed the biodegradable polymer-coated Orsiro sirolimus-eluting stent (SES; Biotronik) and the biodegradable polymer-coated Synergy everolimus-eluting stent (EES; Boston Scientific) versus the durable polymer-coated Resolute Integrity zotarolimus-eluting stent (ZES; Medtronic). The study was performed in four centres in the Netherlands between December 2012 and August 2015 and enrolled 3514 all-comer patients who required PCI with DES implantation. Inclusion and exclusion criteria were kept broad to ensure enrolment of an all-comer patient population. All coronary syndromes were permitted, and no restrictions were set for lesion length, reference vessel size, number of lesions, restenotic lesions or coronary bypass lesions. Patients were randomly assigned (1:1:1) to treatment with the SES, EES or ZES. All patients provided written informed consent. The trial complied with the Declaration of Helsinki and was approved by Medical Ethics Committee Twente and the institutional review boards of all participating centres.
PCI was performed according to current medical guidelines and the operator’s judgment. Clinical follow-up was obtained for up to 3 years, during visits to outpatient clinics, by telephone follow-up or via questionnaire. Research staff members were blinded to the assigned stent type. There was no routine angiographic follow-up. No health economic analysis plan was designed prior to the study. In the current analysis, we aimed to compare health effects and costs of three DES (SES, ZES and EES) from a health insurer perspective in the Netherlands. The 3-year follow-up data of patients with obstructive coronary artery disease, who were percutaneously treated with the three different stents, were retrospectively used for the analysis.
2.2 Health outcomes
In this study, health outcomes were reported as the number of adverse cardiovascular events and quality-adjusted life years (QALYs), i.e., the utility (numerically representing the quality of life) of a health state multiplied by the time being in that health state. Cardiovascular events after PCI were reported per 1000 life years per treatment strategy (i.e. per stent type) for up to 3 years of follow-up. Cardiovascular events included myocardial infarction, major and minor stroke, mortality and repeat revascularisation by means of PCI or coronary artery bypass graft surgery (CABG). Except for mortality, all consecutive events were recorded: hence, a single patient could experience several adverse cardiovascular events of the same event type. Events were prespecified according to the definitions of the Academic Research Consortium [10, 11].
In the BIO-RESORT trial, patients did not complete health-related quality of life questionnaires such as the European Quality of Life Five Dimension Five Levels (EQ-5D-5L). Therefore, utilities were based on previous studies (Table S1). We used the Cost-Effectiveness Analysis Registry [12] to search for utility decrements for each cardiovascular event and chose values from populations that best resembled the BIO-RESORT trial participants.
The utility decrements for each event type were validated by consensus between a senior clinical researcher/cardiology resident (E.H.P.) and an expert clinical researcher/ interventional cardiologist (C.v.B.). For repeated revascularisation and myocardial infarction, utility values were obtained from studies that used the EQ-5D-5L questionnaire in comparable patient populations with obstructive coronary artery disease [13, 14]. For major and minor stroke, utility values were based on estimates from studies that assessed disability after stroke [15]. Utility decrement was temporary for repeat revascularisation: it was 30 days for PCI and 90 days for CABG. Additionally, the utility decrements for myocardial infarction and stroke lasted for a year. In the case of several adverse events occurring at the same time, the utility decrement accumulated according to the defined values for each separate event. Death resulted in a utility value of 0. Baseline utility for patients requiring PCI was set at 0.85 [16].
2.3 Costs
Costs of events were determined in retrospect. Data on costs of PCI and cardiovascular events during follow-up were retrieved from the initiating study site, that is, Thoraxcentrum Twente in Enschede, the Netherlands, using the registered financial codes per patient (i.e., the diagnosis treatment combinations). This represented the costs of more than a third of all trial participants (N = 1375/3514; 39.1%). Costs were retrospectively determined from 2014 and 2015, and subsequently indexed to 2020 costs using the Dutch consumer price index. For the health economic evaluation, a health insurer perspective was used. Costs included those of the index procedure, hospital length of stay, diagnostic tests, Heart Team discussion, visits at out-patient clinics, (cardiac) rehabilitation and repeated revascularisation with PCI or CABG. As costs per stent depend on annual local purchase agreements and were comparable for the three DES, we assigned equal costs to each PCI procedure regardless of the stent choice. Costs were reported per diagnosis treatment combination code, that is, the costs per entry in the financial registration system by physicians. To filter out unrealistic costs in the diagnosis treatment combination codes (major outliers), the following thresholds were applied: all costs had to be more than €1, costs for hospital admission had to exceed €1500 and costs for PCI or CABG had to exceed €3000. Costs per cardiovascular event were assigned to trial participants from other hospitals. A detailed overview of cost per event can be found in the Supplementary Material (Tables S2–S3).
2.4 Analyses
The main endpoints of our analysis were differences between stent treatments in both QALYs and costs. A fully incremental analysis was performed in R (version 4.2.1) [17], comparing all three stent treatment strategies with each other. Bootstrap outcomes were used to describe the results. The mean of total life years, QALYs and costs per treatment strategy were calculated. Incremental costs were divided by incremental QALYs as the incremental cost-effectiveness ratio (ICER; i.e. difference in cost/difference in health effects). During the 3-year follow-up, some data could not be collected due to consent withdrawal or loss to follow-up (121/3514 patients; 3.4%). To account for the missing data, we performed two separate analyses. The first analysis comprised a complete case analysis in which only the participants without any missing data were included in the analysis and all participants with any missing data were excluded. In the second analysis, all participants (regardless of any missing data) were included in the analysis. In the latter analysis, for patients with missing data, follow-up was censored at the time of last contact or at the time of consent withdrawal. Patients who withdrew consent allowed for use of their data collected before the time of consent withdrawal. To account for potential impact of differences in baseline characteristics between intervention and control groups on the incremental health effects and incremental costs, a seemingly unrelated regression was performed [18, 19]. All potentially relevant baseline variables were identified as such by expert clinicians (E.H.P., R.A.B. and C.v.B.) by plenary discussion. These variables were included in the seemingly unrelated regression. Moreover, correlations between parameters included in the seemingly unrelated regression are also accounted for in the analysis. Parameters that were taken into consideration in the seemingly unrelated regression for both costs and health effects were: stent type, age, sex, body mass index, peripheral artery disease, diabetes, hypertension, hypercholesterolemia, smoking, previous myocardial infarction, previous stroke, previous PCI, previous CABG, left ventricular ejection fraction < 30% and renal insufficiency. The discount rates were 1.5% for health effects and 4% for costs, in accordance with Dutch guidelines for economic evaluations [20].
2.5 Uncertainty analysis
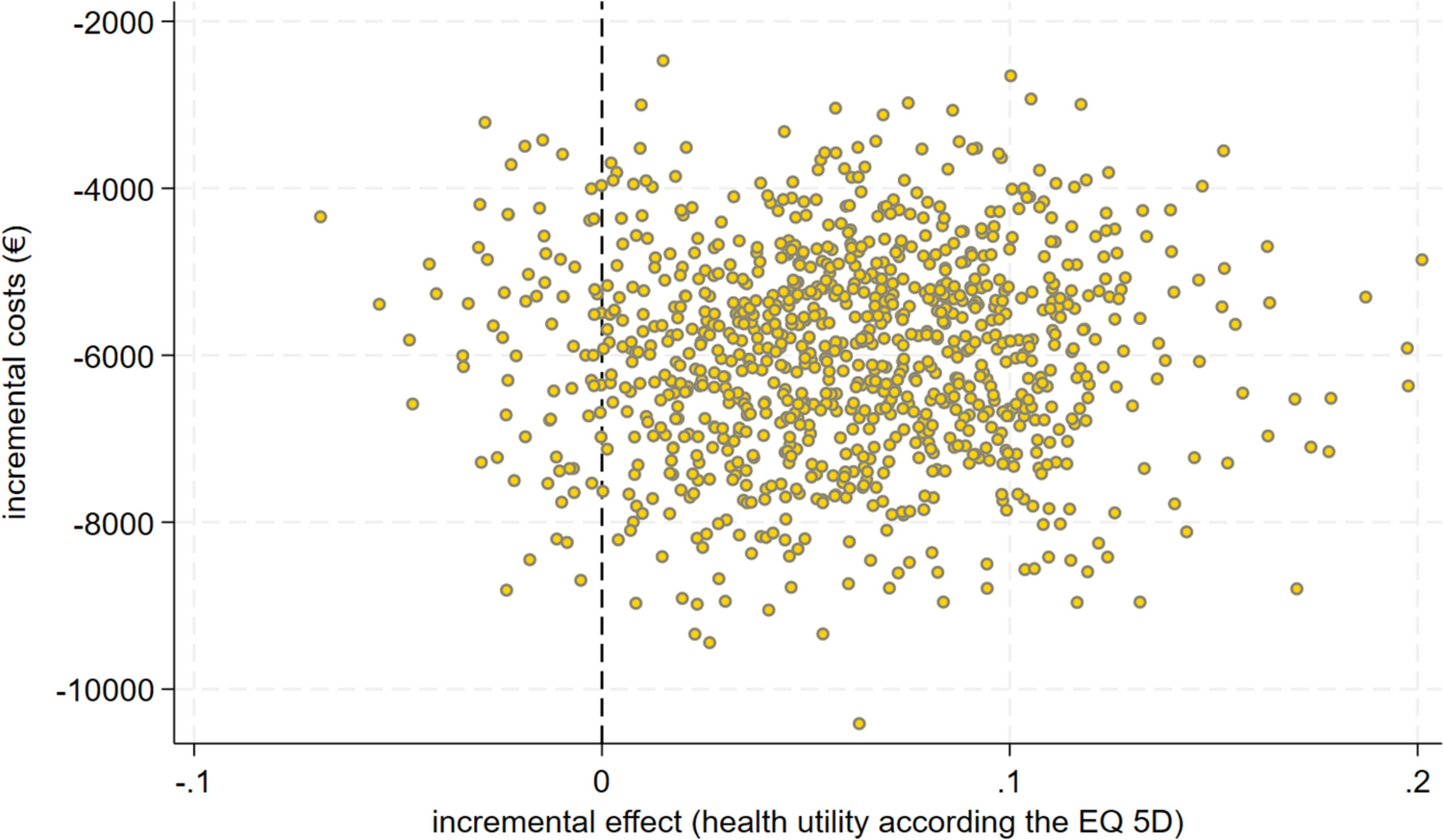
Even though a relatively large study population was included, it is likely that the study population does not perfectly resemble the actual total patient population. Therefore, the uncertainty in costs and health effect outcomes was assessed by means of bootstrapping (5000 iterations with replacement), meaning that the original sample was resampled 5000 times. The mean number of events per stent treatment per year of follow-up based on the bootstrap samples is displayed in Table S4. The seemingly unrelated regression was performed during every bootstrap, and outcomes were calculated in each bootstrap sample. The results were plotted in an incremental cost-effectiveness plane and as cost-effectiveness acceptability curves. The cost-effectiveness acceptability curves represent the probability that each stent is cost-effective over different willingness-to-pay thresholds, which are costs that one is willing to pay for one additional QALY (on a population level). We reported the probability of the stent treatment with the most optimal ICER in the base case analysis of being more effective, cheaper and both more effective plus cheaper (as compared with the other stents) by comparing costs and QALYs of each stent per bootstrap sample.







留言 (0)