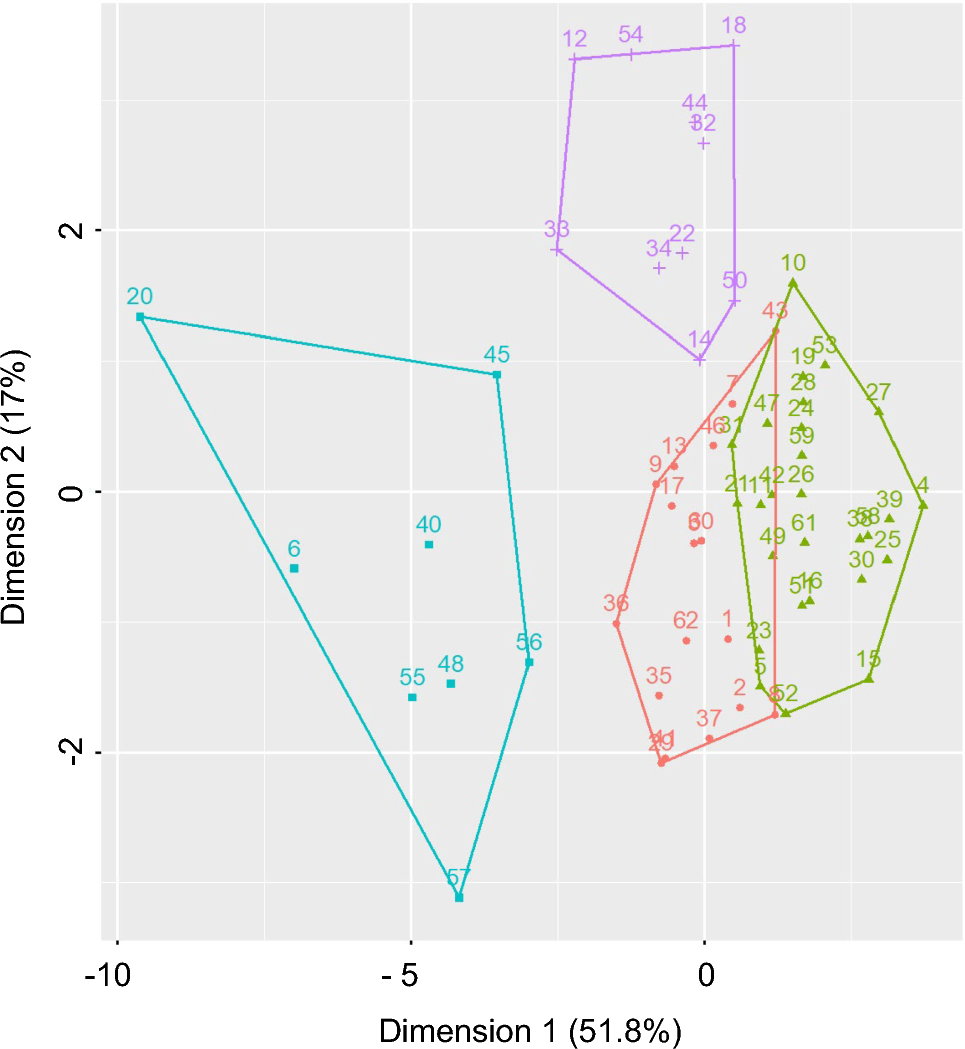
This study identified associations between participants who over-report gastro-intestinal complaints. The implication of over-reporting threatens the validity of research that uses self-report measures for somatic symptoms. To investigate these subjective gastrointestinal complaints, cluster (K-medoid) analysis was applied to MMPI-2-RF results provided by 62 participants. The optimized cluster analysis (Fig. 1) revealed 4 distinct sub-cohorts ranging from 8 to 27 participants per cluster. Once separated into clusters, mean and median MMPI-2-RF scores were calculated for each cluster (Table 3), with categorization for Rome criteria along with responses to a health—wellness questionnaire also defined by individual clusters (Table 5).
Clusters 2 and 4 mean/median MMPI-2-RF scores were not elevated above 65, with cluster 1 having > 65 for GIC only. Cluster 3 was characterized by clinically significant MMPI-2-RF scores for emotional and thought dysfunction, somatic and gastrointestinal complaints, and suicidal ideation. However, caution is required for cluster 3 MMPI-2-RF results as scores were also elevated for the validity scale FBS-r, which indicate infrequent reporting and somatic and cognitive complaint over-reporting. These issues in reporting somatic and GI complaints question the validity of self-reported GI symptoms from participants with certain personality profiles and/or psychopathology, and level of somatization versus physically explained GI symptoms. The MMPI-2-RF results for cluster 3 participants support research by Aparcero et al. [29] that showed participants with personality and psycho-pathological challenges are more likely to feign or exaggerate their symptoms compared to healthy participants.
One possible explanation for our results is that personality profiles and/or psychopathological disorders, characterized by low tolerance for distress and excessive rumination of problems, will distort symptom reporting [30,31,32]. Somatization, meaning psychological distress manifested as physical symptoms, have been found to exist in research measuring linkages between GI symptoms and MMPI assessed personality and psychopathological symptoms [13]. Multiple studies have found somatic disorders to exist in Rome Criteria-assessed FGIDs [33,34,35] but have not questioned the validity of the self-reported GI symptom scales to determine the level of somatization versus physically based symptoms.
The MMPI-2-RF’s validity scales offer an objective measurement of self-reported GI symptoms and somatization [36], which was extended by this investigation through understanding MMPI-2-RF response structures via cluster analysis and whether response validity requires deeper consideration. A meta-analysis [29] found that MMPI-2-RF validity scales effectively separated accurate participant responses from participants who feigned or exaggerated psychological or medical symptoms. Specifically, the embedded Fs validity scale detects infrequent somatic responses in contrast to the FBS-r validity scale that detects non-credible symptoms [29].
In relation to GI symptoms, emotional dysfunction, such as stress, anxiety, and depression, have been observed to exacerbate GI symptoms [1, 2]. Because of psychological stress’s influence on FGID development and GI symptoms, it is essential to detect somatization early to prevent or reduce the exacerbation of GI symptoms [1, 37] and to guide treatment decision-making. Future research should assess self-reported GI symptoms in conjunction with measures of somatization [29] and consider psychological interventions as early treatment for FGIDs [37].
Our study found that the report of GI symptoms correlates with certain (high order) dysfunction types and with specific symptoms of psychopathology, but that distress may need to be interpreted with caution because of over-reporting. The cluster results emphasized the need to stratify MMPI-2-RF results that had the greatest elevation of scores pertaining to both IBS and psychopathology and as suggested by clinical history, were also more likely to have an altered gut homeostasis because of other factors, such as allergy, autoimmune disease, or the prescribing of psychotropic medication (results not shown).
While physiological GI tests, such as microbiome testing, can directly explore questions of causation and thereafter propose appropriate treatments for GI symptoms and FGIDs [1, 38], GI and somatic symptoms and disorders are often measured via self-report surveys because they are a more accessible and affordable option [23, 39]. Therefore, it is essential that self-reporting is optimized. The results of this investigation emphasized issues in self-reporting as determined via MMPI-2-RF validity scales revealed by interrogating the cohort data structures by K-med cluster analyses. In short, the physical complaints reported by some participants may have no identifiable physiological foundation and as such need to be considered when assessing participants. This may ultimately include the role of somatization in increasing the rate of gastrointestinal complaints in those with psychopathology or personality disorders.
The primary limitation of this investigation was the small number of total research participants that resulted in smaller sample sizes for the separate clusters that were the focus of deeper examination. This was a particular problem for cluster 3 with only 8 participants but representing several MMPI-2-RF features of interest to our aims. Small sample size introduces the risk of inadequate statistical power (1 − β), which for the ANOVA results (Table 3) were often compensated for by large effect sizes. However, despite large effect sizes, some ANOVA results did not achieve statistical power of greater than 0.80 (range: 0.102 to 0.996), suggesting caution for the interpretation for some results. For noting within this limitation, Standard Error of the Mean (SEM) values were less than 10% of the mean across all clusters, except Fs in Cluster 3. Cluster sample size was also a challenge for the statistical investigation of the Rome criteria and the role of other self-reported health factors (Table 5). To address this limitation Fisher’s exact probability was calculated, rather than the p value estimated via standard Chi-Square.
As well as sample size, the cohort investigated represented a community convenience sample that may suggest self-selection bias. To address these limitations the study relied upon the application of validated measurements of personality/psychopathology (MMPI-2-RF) and gut disorders (Rome Criteria) to a new Australian participant cohort, whose assessment also included a clinical questionnaire to detect biases. To augment the rigor provided by these validated instruments, an unsupervised cluster algorithm was applied to define distinct MMPI-2-RF response sub-cohorts and link these to other measures of GI and general health, with implications for the deeper understanding of factors that cause gut dysbiosis, and to ultimately assist the treatment of mental health disorders in the context of self-reporting veracity independent of location.
The results of this investigation provide a quantitative method to reveal patterns contained within MMPI-2-RF response profiles that will assist in the evaluation of reporting veracity and therefore improved health assessment. In this context, the embedded validity scale FBS-r was valuable and linked to suicidal ideation (SUI), as well as other markers of psychological distress. The relationship between suicidal distress and IBS has been previously noted [40, 41]. This distress is perceived as significant by the responder and importantly, not only impacts the way in which symptoms are related, but also the behavioral response to those symptoms.
Considering these results, we speculate that gut dysbiosis can impact personality, which leads to low tolerance for distress and heightened somatic focus on gut symptoms. This was reflected by cluster 3, which combined elevated responses for a number of psychological—personality dysfunctions, gut symptoms (GIC), and also elevated responses to internal validity scales within the MMPI-2-RF. Applying the cluster methods developed herein, subsequent studies will request fecal samples from participants to screen for gut dysbiosis, to explore whether the results obtained via survey questionnaires and psychological instruments are reflected physiologically via microbiome aberration.


留言 (0)