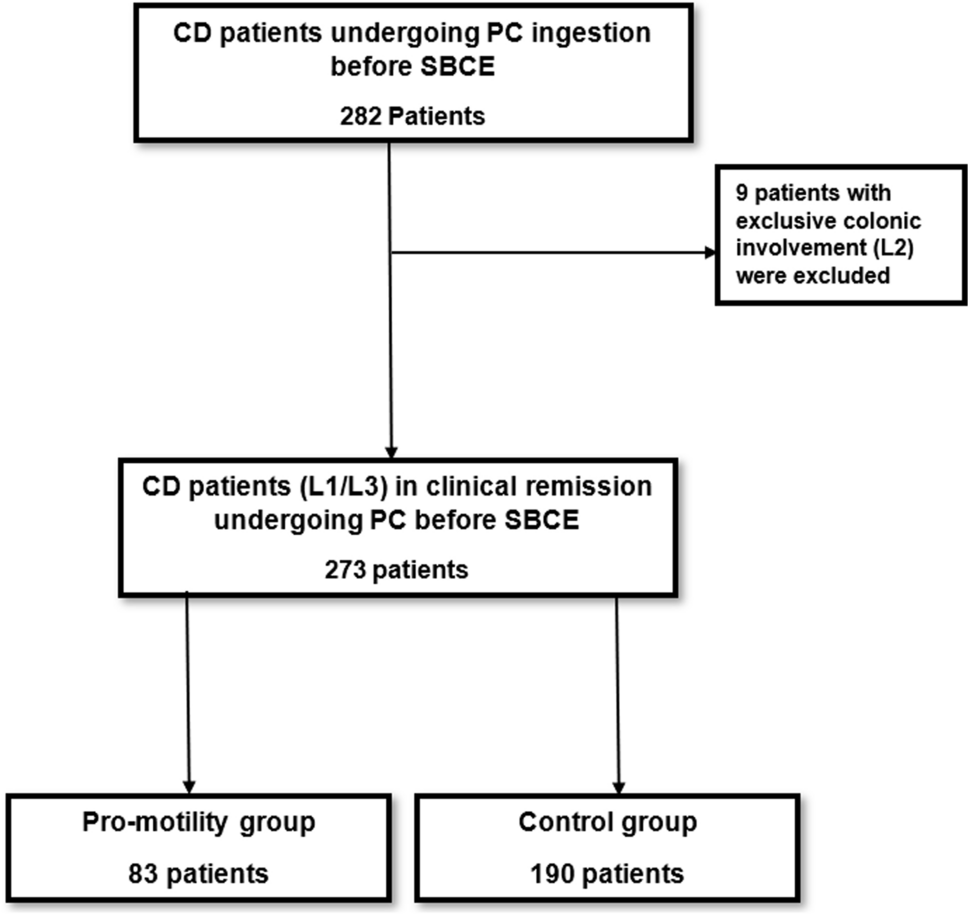
In this retrospective bi-center study, we compared, for the first time, two different preparation protocols before PC ingestion among patients with CD in clinical remission. We found that in this population, a pro-motility preparation protocol based on a low-residue diet followed by clear fluids and post-capsule-ingestion bisacodyl was superior to a clear fluid-diet alone for reducing the rates of failed PC events and increasing the successful patency test of the SB. Moreover, longer disease duration was associated with an increased risk of failed PC, while the use of the pro-motility preparation protocol prior to and during PC ingestion was associated with more than a 50% reduction in the probability of failed PC in this population, overshadowing other risk factors, including B2/3 disease phenotype and previous CD-related surgery.
Mucosal healing (MH) is a paramount goal in the management of patients with CD, as it has been linked to improved long-term outcomes in this population [24]. In light of the substantial rate of patients with CD who have exclusive SB disease involvement (~ 30%), the role of SBCE has become crucial in accurately evaluating MH in CD [1]. SBCE has been proven to be a useful tool in diagnosing and monitoring patients with CD and in identifying future disease adverse events, among them [4, 20, 25,26,27]. However, its use is limited by the potential risk of capsule retention, which may lead to self-limiting mild symptoms or serious complications such as SB obstruction or perforation, resulting in emergent surgery [8]. SB patency confirmation before SBCE ingestion has led to reduced capsule retention rates by 50–70% among patients with established CD [5,6,7,8,9]. Therefore, both US and European guidelines endorse the assessment of SB patency prior to SBCE ingestion in patients with CD [10, 11].
The use of PC in patients with CD has been proven to accurately screen out patients at high risk for retained SBCE [13, 14], and it has a higher negative predictive value (NPV) compared to MRE in assessing SB patency in CD[15]. We also demonstrated its predictive yield for future adverse events in patients with quiescent CD [28]. Yet, the PC procedure has a considerable rate of FP results (i.e., 55–87%) among patients undergoing the procedure before SBCE for any reason (i.e., CD assessment and diagnosis, gastrointestinal bleeding, polyp follow-up, etc.) [16,17,18,19], leading to insufficient positive predictive value (PPV) for evaluating SB patency [16,17,18,19]. Previously published studies found a non-significant association between constipation and failed PC [16, 17]. However, in an analysis restricted to patients with FP results of failed PC (n = 24), constipation was the only factor that independently increased the probability of failed PC (OR 13.858, p = 0.042) [16], while it had no influence on SB patency confirmation based on a two-step assessment process (i.e., PC ingestion → cross-sectional imaging) [16, 18]. It is, therefore, conceivable that PC excretion time might be delayed (≤ 72 h) and still represent intact SB patency [13].
Notably, in our study, colonic involvement was more prevalent in the control group compared to the pro-motility group. Colonic disease involvement in CD can result in either diarrhea [29] due to inflamed mucosa or constipation with delayed transit time due to colonic strictures [30], which may hinder PC excretion in these patients. However, no association between colonic disease involvement and the risk of failed PC was demonstrated. Unfortunately, data regarding bowel movement habits in the cohort population were unavailable, limiting our understanding of the impact of colonic involvement on PC results.
In our study, we observed that patients with CD in clinical remission who followed the pro-motility preparation protocol had a lower rate of failed PC compared to controls who followed the fluid-only preparation protocol. This finding contrasts with a previously published study, which found no association between the use of prokinetics and the likelihood of failed PC among patients who underwent PC ingestion for any indication [16]. However, practical conclusions from that study were limited by the low prevalence of prokinetic use in its study population (5.67%) [16]. Interestingly, we found that the pro-motility preparation protocol has a stronger and more significant effect on males (OR 0.209, p = 0.008) compared to females (OR 0.725, p = 0.637). This observation may be explained by the higher prevalence and greater severity of constipation in females compared to males [31]. Considering the above-mentioned findings and the generally comparable baseline characteristics between females and males in our study, these results may indicate the need for a more robust preparation protocol for female patients. Our findings suggest the need for further research to tailor preparation protocols to distinct sub-populations in CD to reduce the rates of failed PC in CD.
Longer disease duration in patients with CD is associated with higher rates of complicated disease phenotypes, progressing from B1 to B2/B3 phenotypes over time [32]. It therefore reasonable that longer disease duration might be associated with an increased risk of failed PC, as demonstrated in our study. Not surprisingly, in the analysis restricted to patients with B2/B3 disease phenotypes, the use of pro-motility preparation protocol did not improve failed PC rates in this population, likely indicating an anatomical rather than motility-related cause for a failed PC event.
Consistent with the existing literature, we found PC ingestion to be a tolerable and safe procedure, with only one patient experiencing self-limiting mild symptoms following the procedure. Abdominal pain after PC ingestion was reported in 2/326 patients (~ 0.6%) in a recently published study [17]. Older studies reported higher rates (10–22%) of abdominal pain following PC ingestion; however, in most of those studies, patients had a prior history of symptomatic strictures, unlike the patients in our cohort who were in clinical remission. Our study further strengthened the value of the PC procedure in preventing SBCE retention. We observed only a single case of SBCE retention following a failed PC result (0.4%), which was consistent with the reported rates (0.39–2.1%) [12, 16, 18] of this complication in patients with confirmed SB patency by PC. In contrast, the reported rates of capsule retention were much higher in patients with a failed PC result (11.1%) [12].
This study had several limitations, primarily due to its retrospective design. First, there were no data regarding bowel movements, exercise habits, or daily fluid intake among the study population, which might have influenced PC passage through the SB. However, the cohort was relatively homogenous, consisting of adult patients with CD in clinical remission. Second, the unbalanced higher rate of B2/3 disease phenotype in the control group, along with the higher median age in the pro-motility group compared to the control group, may have influenced the observed failed PC rates. However, in a logistic regression analysis incorporating both variables among others, the use of the pro-motility preparation protocol was still independently associated with a reduced likelihood of a failed PC event. Finally, no cross-sectional imaging was performed following PC ingestion among the study patients, so we could not assess the true FP rates of failed PC or how these rates were affected by the pro-motility preparation protocol. Moreover, cross-sectional imaging is not typically performed following a failed PC event in real-life practice for patients with CD, and there are no guidelines to endorse this approach.
In conclusion, in this bi-center study, we compared, for the first time, two different preparation protocols before PC ingestion among patients with CD in clinical remission. The failed PC rates were significantly lower with the pro-motility preparation protocol, which included a low-residue diet, fluid diet, and bisacodyl, compared to a clear fluid-only diet. Furthermore, longer disease duration was associated with an increased risk of failed PC, while the use of the pro-motility preparation protocol was associated with a decreased likelihood of a failed PC event. Therefore, the pro-motility preparation protocol should be considered prior to PC ingestion in patients with CD in remission to reduce failed PC rates in this population. Further research with a larger cohort is needed to explore this observation more thoroughly and to tailor bowel preparation protocols more effectively for distinct populations with CD.


留言 (0)