
記住我





We performed a retrospective cohort study that included 50 hospitals (48 after propensity score matching) using data from the PHIS database, an administrative and billing database maintained by Children’s Hospital Association (Lenesa, Kansas and Washington, D.C). The PHIS database contains deidentified clinical and resource utilization data for inpatient and outpatient encounters at United States children’s hospitals. Data quality is monitored by the Children’s Hospital Association which issues quarterly reports, chart audits, and feedback to participating hospitals. Institutional review board approval was obtained from Children’s Hospital Los Angeles.
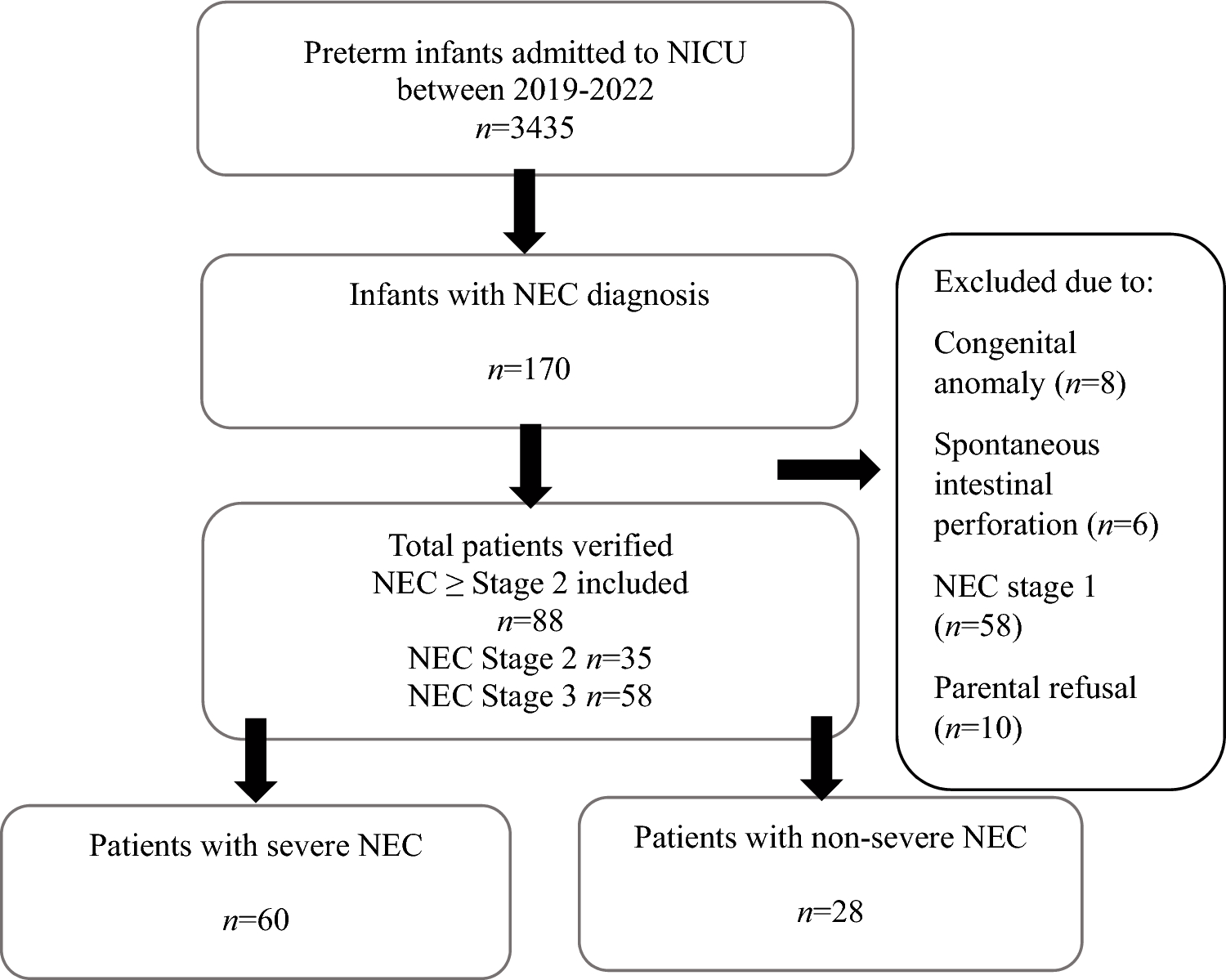
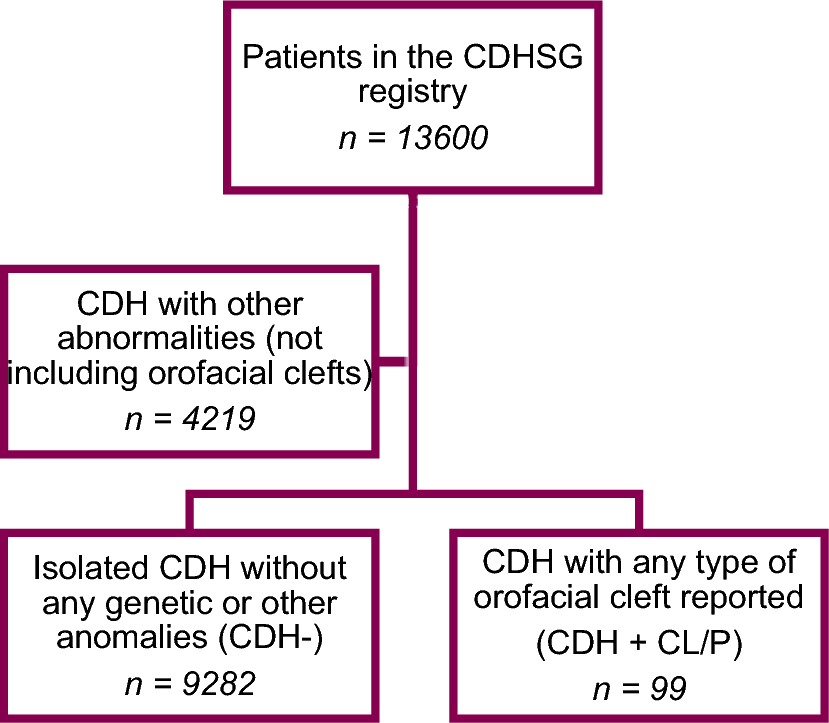
Our study cohort included children aged 21 years or younger who had both a diagnosis of appendicitis and underwent appendectomy, admitted between 3/19/2020 and 7/31/2022. Our start date was chosen based on when the first state issued a stay-at-home order. Children with pre-hospital ventilation needs, supplemental oxygen needs, or who expired were excluded from the study (Fig. 1). Additionally, children with missing Child opportunity (COI), all patients refined diagnosis-related groups (APR-DRG) illness severity score, sex, or race data were also excluded. Children with chronic respiratory disease and who had cardiac arrest were excluded as there were no children with COVID-19 with whom to match them.
Fig. 1
Patient selection flowchart
Outcome measuresOur primary outcome measure was hospital length of stay. Our secondary outcomes included incidence of ventilation and ventilation days, 30-day re-admission, 30-day mortality, and intra-peritoneal drain placement identified by current procedural terminology (CPT) codes 44,900 and 44,901.
CovariatesDemographic characteristics included age at admission, patient admission type, sex, race, ethnicity, insurance type, hospital region, Child opportunity index (COI), presence of a complex chronic condition [14], and APR-DRG illness severity score. Patient admission type included inpatient, emergency department visit, ambulatory surgery, or observation unit. Race categories included Asian, Black, Other, and White. “Other” race was defined as Native Hawaiian/Pacific Islander, American Indian, and Alaska Native. Insurance type was categorized as private (commercial plans, TRICARE, military insurance), public (Medicare, Medicaid, Children’s Health Insurance Program), and other (any other government insurance, self-pay, charity care, any insurance not previously mentioned).
Children with COVID-19 infection during hospitalization were identified using the International Classification of Diseases, Tenth Revision (ICD-10) codes U07.1 and U07.2. Data extraction from the electronic medical record via chart review was performed on the 555 patients at our institution to assess PHIS’s COVID ICD-10 coding accuracy. We found that PHIS ICD-10 coding reported COVID with 98% accuracy, 100% positive predictive value, 97% negative predictive value, 54% sensitivity, and 100% specificity. These numbers are similar or better than previously published studies [15, 16]. A total of 28 children who tested positive for COVID-19 prior to surgery, and we identified 13 patients who had preoperative COVID diagnoses that PHIS did not identify. Of those 13 patients, 8 did not have COVID ICD codes attached to their encounter, and 1 patient was likely a false-positive test as they tested negative 24 h later.
Diagnosis of appendicitis was identified using ICD-10 codes K35, K35.3, K35.30, K35.31, K35.8, K35.80, K35.89, K35.890, K35.891, K36, and K37. Perforated appendicitis was identified by ICD-10 codes K35.2, K35.20, K35.21, K35.32, and K35.33 [17]. Appendectomy was identified using ICD-10 procedure codes 0DTJ4ZZ and 0DTJ8ZZ for laparoscopic surgery, and 0DTJ0ZZ and 0DTJ7ZZ for open surgery.
Pre-hospital ventilation needs were defined by ICD-10 code Z99.11 and supplemental oxygen needs were defined by ICD-10 code Z99.8. Children with chronic respiratory disease were identified using ICD-10 codes G47.35, I27.82, I43, J84.112, J96.20, and Z90.2. Children who had cardiac arrest were identified using ICD-10 codes I97.121 5A12012, 5A1221Z, and 5A2204Z.
The Child opportunity index (COI) 2.0 is a composite index of 29 indicators of neighborhood resources important to healthy childhood development across three domains: education, health and environment, and social and economic [18]. For this study, COI was measured at the zip code level. Each zip code is assigned a nationally normed neighborhood opportunity score from 1 (lowest) to 100 (highest), and is further categorized into COI quintiles (very low, low, moderate, high, and very high opportunity). The COI is administered by diveresitydatakids.org at the Institute for Child, Youth and Family Policy at the Heller School for Social Policy and Management at Brandeis University (Waltham, MA). [19]
The APR-DRG illness severity score was developed by 3 M Health Information Systems as a measure of illness severity based on clinical similarities and use of hospital resources to compare outcomes across hospitals [20]. Severity classifications include minor, moderate, major, and no class specified.
Statistical analysisCategorical variables were described using frequencies and percentages, and continuous variables were described median and interquartile range. Chi-square tests for categorical variables and Mann–Whitney U tests for continuous variables were used to compare differences between groups. Given the significant difference in sample size and observed covariates between COVID negative and COVID positive patients, we used propensity score matching to select similar patients for comparison postoperative outcomes. Greedy (1:1 ratio) propensity score matching was performed to match the study group. Patients were matched on age, sex, race, ethnicity, patient admission type, insurance type, Child Opportunity Index, surgical approach, perforation status, hospital, all patients refined diagnosis-related groups (APR-DRG) illness severity, and presence of a complex chronic condition. We felt it necessary to match on race and ethnicity, insurance type, and COI given previous studies demonstrating that children from racial and ethnic minorities [21,22,23,24,25], children with low socioeconomic status [26], and children with public insurance [22, 25] are at higher risk for perforated appendicitis, and therefore at higher risk for complications [27]. All statistical significance tests were conducted with a two-sided α = 0.05. Matching and data analysis was done using SAS software (SAS Institute, Inc, Cary, North Carolina).
留言 (0)