Key findings
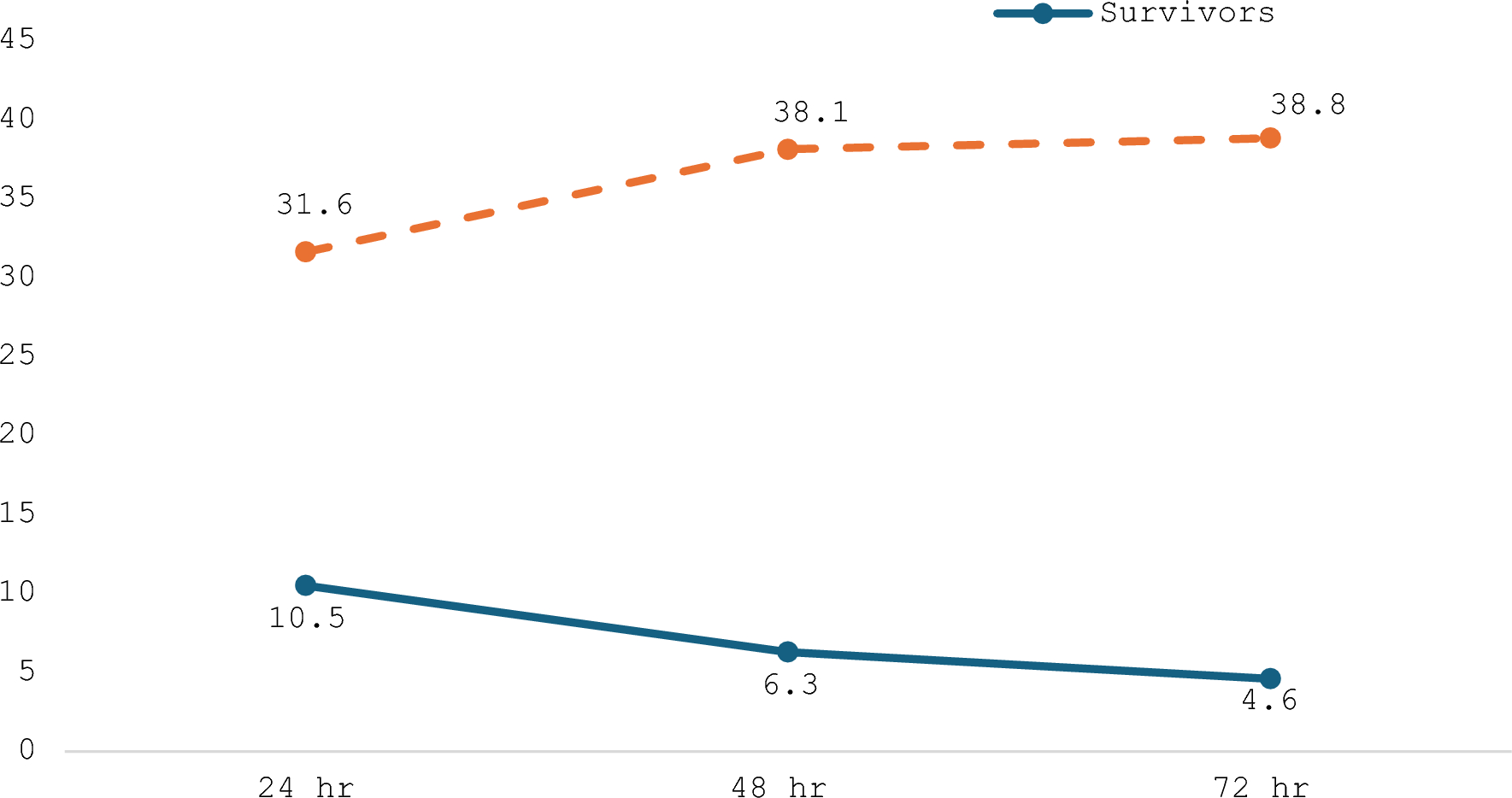
In 2018, surgical management of HSCR was centralized from four to two centers in Sweden. This retrospective, multi-center study aimed to assess the early postoperative outcomes following centralization of care for HSCR. Surgical management shifted, with an increase of laparoscopically assisted endorectal pull-through (8.8% to 39.8%). No significant differences were seen in postoperative hospital stay, unplanned procedures under general anesthesia or readmissions up to 90 days after pull-through. Severe complications (Clavien–Madadi ≥ 3) up to 30 days after pull-through did not differ between the time periods. HAEC treated with antibiotics increased following centralization (10.5% to 24.1%).
Interpretation
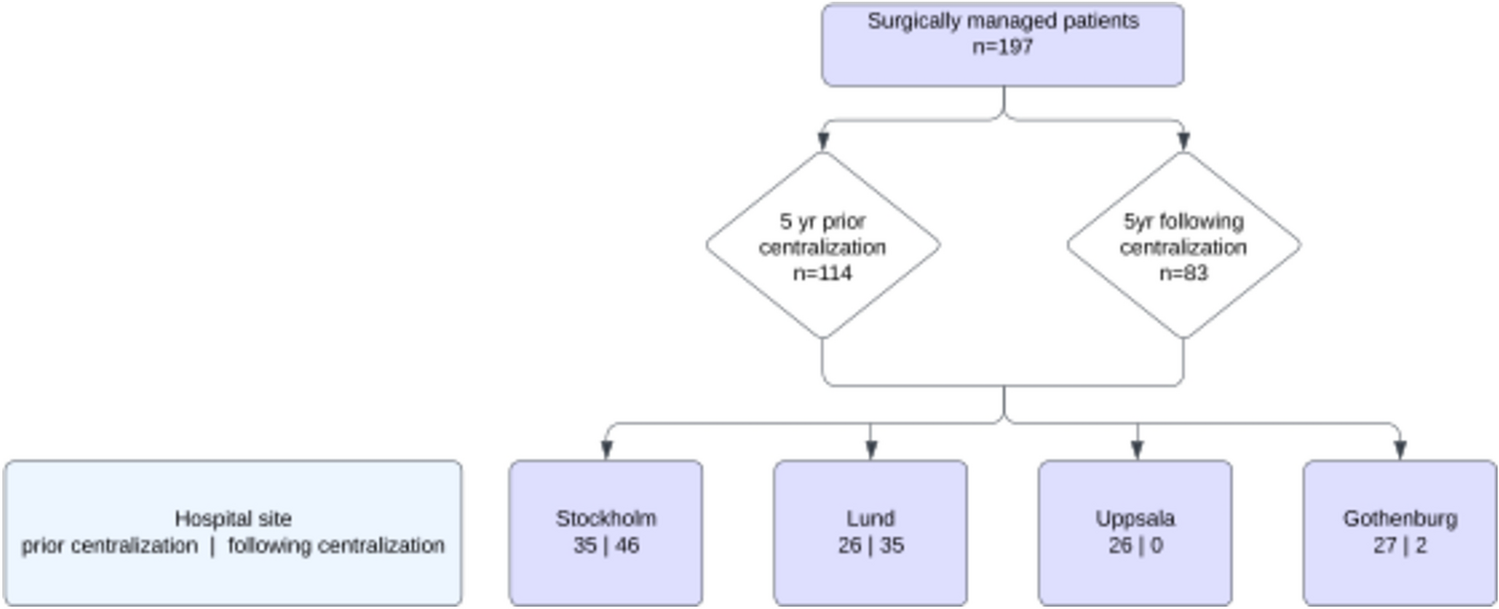
From initial diagnostics to early postoperative outcome, few changes were observed following centralization. There was a 27% reduction in patients from 114 in the 5 years prior to centralization to 83 in the 5 years following centralization. This might partially be accounted for by declining birth rates and a higher proportion of children being born in the spring and summer months. From 2013 to 2018, a mean of 115 341 births per year was recorded compared to 110 413 births per year 2018 to 2023. Birth rates in 2023 were the lowest recorded during the time period, only 100 051 [13]. Furthermore, some patients born in 2023 with late diagnosis or postponed surgical treatment may have been excluded, as only patients who had undergone definitive repair the 30th of June were included.
There were no differences in age at biopsy, need of re-biopsy, age at diagnosis or time from diagnosis to pull-through between the time periods. With fewer centers, the travel distance to treating hospital increased for many patients following centralization. There are studies indicating a higher risk of delay in diagnosis and misdiagnosis in patients residing at longer distance to the tertiary referral hospital. This concern may be even higher in patients with rare diseases [14, 15]. Therefore, it is crucial that our results do not indicate such disparities, ensuring accurate and timely diagnoses despite patients living more distant to the referral hospital.
Surgical technique differed prior to and following centralization. The most noteworthy being an increase in laparoscopically assisted pull-through from 8.8% to 39.8%. Trananal endorectal pull-through remained the most commonly performed procedure, 65.8 and 43.4%, prior to and following centralization. Although these findings are interesting and probably reflects a change in the general trend of HSCR treatment in Sweden, it seems unlikely to have been an effect of centralization nor impact the results as all procedures are considered feasible and safe without evidence supporting superiority in outcome for either [16].
Although volume-outcome benefit for complex surgery is widely recognized [17,18,19], results of our study did not show a reduction of postoperative complications, unplanned procedures or unplanned readmissions following centralization of care. Many studies favoring centralization consider high-risk procedures with considerable short-term morbidity as well as complex procedures for conditions with high mortality. In high-income countries, HSCR mortality rates are low, while long-term morbidity remains a pressing issue [20,21,22,23]. This may reflect why our results, considering only short-term outcome, does not show any significant improvement in outcome. The number of patients managed in each center is low also after centralization, which is important to take into account when the results are interpreted. It could be argued that the potential advantages of centralization require larger volumes.
HAEC requiring treatment with antibiotics increased from 10.5 to 24.1%. Although noteworthy, this rise might be attributed to increased awareness of mild HAEC cases managed at home with oral antibiotics and transanal irrigations. There does not seem to be differences with respect to incidence rate of residual aganglionosis or anastomotic strictures, that could potentially explain the increased HAEC incidence. We have previously shown at our center that at-home transanal irrigations, although utilized during the preoperative course, remains a safe and adequate mode of decompression despite living far from the index hospital [11]. In addition, the threshold for initiating treatment might be lower in patients who do not have easy access to the index hospital, as a form of safety precaution. Unfortunately, we cannot determine the true cause of the reported increase in HAEC, as no grading of severity or symptoms was conducted.
Limitations
Results of this study should be considered with regards to several limitation. The retrospective design of the study may impact the accuracy of the collected variables. Since multiple individuals collected the data, there is a risk of inconsistent interpretation of reviewed variables. In addition, the limited size of the HSCR cohort affects the study’s power and increases the risk of type II errors. Comparing patients from two different time periods and different hospitals may also introduce confounding factors, such as changes in senior staff, new procedures or protocols, and evolving scientific evidence influencing treatment practices.
Generalizability and clinical implications
This is the first study of its kind evaluating the surgical and postoperative course of patients with HSCR following centralization of care. It provides a national oversight of patient outcome following this change of procedure in Sweden and is one of few existing studies evaluating centralization of pediatric surgery.
While our study provides valuable information on the topic of centralization, results should be interpreted cautiously when applied elsewhere. Diagnostic methods and treatment protocols may vary significantly from one country to another. The unique demographic and organizational aspects of Swedish healthcare may also limit the generalizability of the results to other settings. In addition, the implementation of centralization can differ across countries, influencing caseloads, travel distances, and outpatient management. In countries where the number of pediatric surgery centers is high relative to the population, with some centers potentially handling a very limited number of cases per year, the impact of centralizing surgical care may be more significant. In Sweden, before centralization, none of the centers handled less than five patients annually, which enabled these active centers to sustain high-quality care and surgical competence. As a result, centralization may have held lower impact in short-term outcomes than expected.
It is easy to oversimplify the benefits of centralization by assuming that higher case volumes automatically lead to greater surgical skill and fewer complications. However, even with an optimal pull-through procedure, the risk of impaired bowel function and HAEC remains significant [21,22,23]. In addition, between 4 and 30% of HSCR patients have associated developmental disorders or syndromes [16]. Therefore, the ability to manage the entire disease process is just as crucial as the ability to perform complex surgeries. Given this, multidisciplinary teams are essential in providing individualized, holistic care, and the conditions for developing such teams are better in high-volume hospitals [7].
Our results could not show major improvement nor deterioration in the diagnostic course, surgical management, and early postoperative outcome following centralization of care. The reported rise in HAEC rates is a point of observation but has many plausible explanations that do not necessarily relate to worsened outcome.
Further research is needed to assess long-term impact of centralization of HSCR. Studies addressing bowel function, quality of life, and patient and parent satisfaction following centralization are required. There is also a need for international studies with larger cohorts to counteract statistical uncertainty as well as research into multiple aspects of centralized care. Furthermore health-economic analysis and studies looking at the combined total effect of centralization of multiple diagnoses are required. This to secure that centralized care results in better health outcomes, better use of resources, increased competence of surgeons and better conditions for research, education and quality development with regards to these diagnoses.
Conclusion
Centralization of care for HSCR does not seem to delay time to pull-through nor reduce severe complications, unplanned procedures under general anesthesia or readmissions up to 90 days after pull-through. There was an increase in HAEC following centralization, possibly due to increased awareness of mild HAEC.






留言 (0)