
記住我


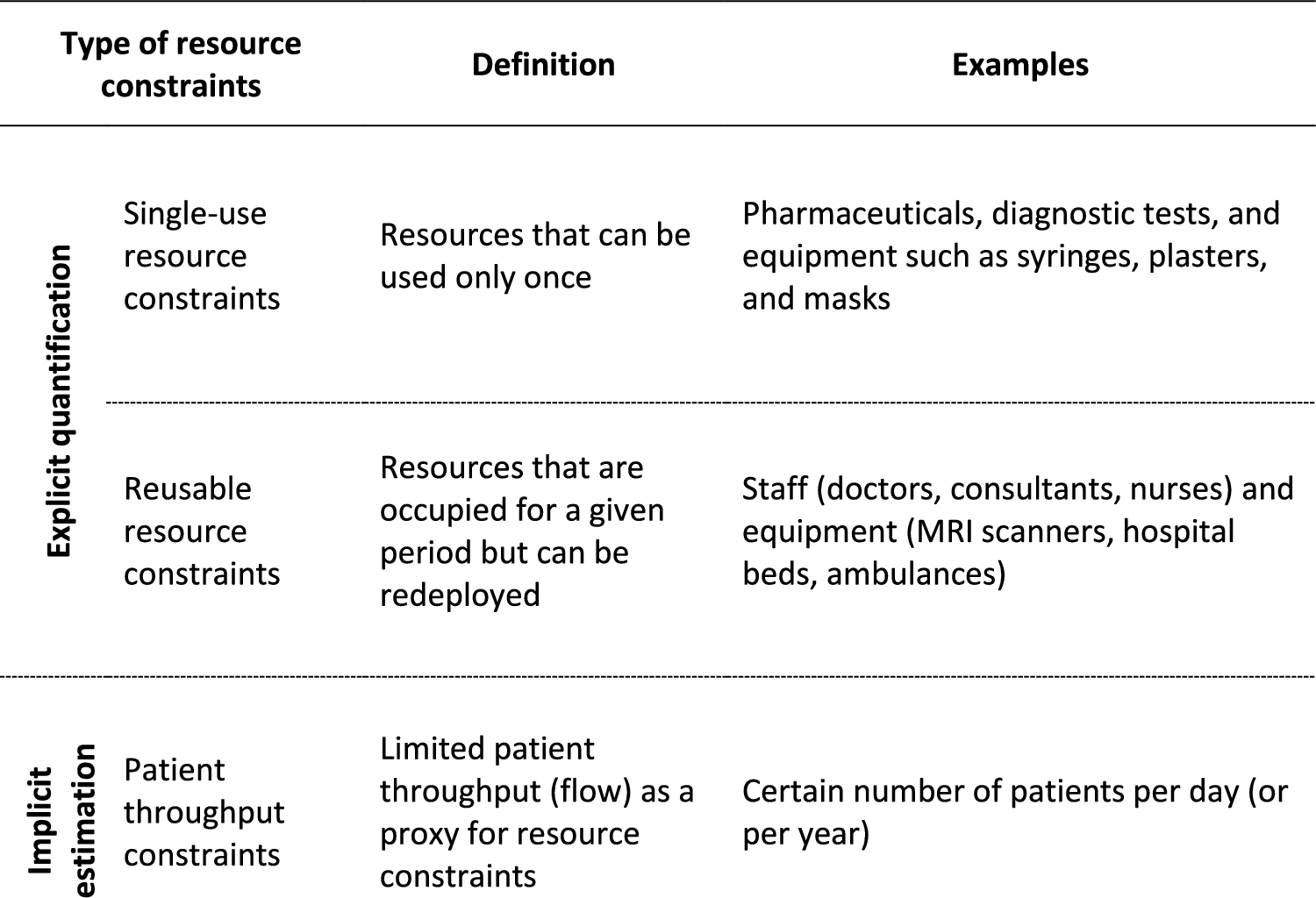




We developed a partitioned survival model consisting of progression-free (PF), progressed (PD), and death to evaluate the cost-effectiveness of fruquintinib (Fig. 1). Given that there is currently no recommended treatment for patients who had disease progression on or had been intolerant to trifluridine–tipiracil and regorafenib, we compared fruquintinib with the placebo, consistent with the FRESCO-2 trial. We estimated life-years (LYs) and quality-adjusted life-years (QALYs) for each group.
Fig. 1
Partitioned survival model to evaluate the cost-effectiveness of fruquintinib versus placebo
The baseline characteristics and clinical outcomes were based on the FRESCO-2 trial [16]. The FRESCO-2 was an international, randomized, double-blind phase 3 trial in which 934 patients were randomized 2:1 to receive fruquintinib or placebo. The trial involved 124 hospitals and cancer centers in 14 countries across North America, Europe, Asia, and Australia. The median age of participants was 64 years old, approximately 55.7% were male, and 80.9% were white. The median number of previous treatment lines in metastatic disease was four in both groups, and the types of treatments were similar. Approximately 52.2% had been previously treated with trifluridine–tipiracil and 39.4% had been previously treated with both trifluridine–tipiracil and regorafenib.
The time horizon of the model was the patient’s lifetime, defined as 10 years, during which most patients in both groups die. The model cycle was set to 1 week to accurately include the various treatment cycles for each drug, including subsequent treatments. We used a discount rate of 3.0% per year for both clinical outcomes and costs [21]. The model was developed using Microsoft Excel (Microsoft, Redmond, WA, USA).
2.2 Clinical InputsWe reconstructed the patient-level data from the PFS and OS curves of the FRESCO-2 trial, using Engauge Digitizer version 12.1 [22] and algorithms from Guyot et al. [23]. On the basis of the reconstructed data, we conducted parametric estimation following the Technical Support Documents in the National Institute for Health and Care Excellence [24]. We checked the proportional hazards assumption using log-cumulative hazard plots and found that PFS met the assumption, but OS did not (Supplementary Fig. 1). Therefore, we used accelerated failure time models to estimate PFS distribution and independent models to estimate OS distribution. Among the Weibull, lognormal, log-logistic, exponential, generalized gamma, and Gompertz distributions, we selected the best-fitted distribution on the basis of the lowest Akaike information criterion and Bayes information criterion, along with a visual inspection of the fit. The proportion of patients in PF, PD, and death for each model cycle was estimated from the best-fitted distribution of PFS and OS curves. We conducted the half-cycle correction on the transition of each model cycle to reduce bias due to transition timing of the population. The estimated PFS was capped by OS, and the estimated OS was capped by the general population mortality in the USA [25]. The R software version 4.3.1 was used for parametric estimation.
2.3 Cost InputsWe estimated direct medical costs from the commercial payer perspective in the USA. Costs for drugs, subsequent treatment, follow-up care, terminal care, and adverse events were included in the model (Table 1). The cost for best supportive care at model entry was not included because the type and proportion of treatment could not be consistently specified for each group. The costs for the drug and subsequent treatment were based on the average wholesale price, obtained from Lexicomp [26]. In the FRESCO-2 trial, patients continued treatment until disease progression, death, unacceptable toxicity, withdrawal of consent by the patient, or discontinuation by the physician. Given our estimation was limited to PFS, we derived the duration of treatment with fruquintinib by applying the ratio of median treatment duration (3.1 months) to median PFS (3.7 months) observed in the FRESCO-2 trial to the estimated PFS. The dosage and regimen of fruquintinib were based on Food and Drug Administration approval, and we applied a relative dose intensity (0.92), which is the actual dose intensity in the clinical trials divided by the projected dose. Types and proportions of drugs used in subsequent treatment were based on the reported data from the FRESCO-2 trial (Supplementary Table 1) [16].
Table 1 Input data for the cost-effectiveness modelCosts associated with follow-up care included costs for complete blood count tests, comprehensive metabolic panel tests, and physician visits, which were obtained from a previous cost-effectiveness study in the USA [27]. Terminal care costs were based on National Cancer Institute data [28] and applied as a one-time cost for the last 3 months of life. To estimate adverse event costs, types and incidence of events were obtained from the FRESCO-2 trial [16], while their corresponding costs were retrieved from a previous US cost-effectiveness study for refractory metastatic colorectal cancer [27]. This prior US cost-effectiveness study derived adverse event costs from the Agency for Healthcare Research and Quality Healthcare Cost and Utilization Project [29], using the same Medicare Severity Diagnosis-Related Groups classification for diarrhea and abdominal pain. Only grade 3 or higher adverse events that occurred in more than 2% of patients were considered. We applied adverse event costs as a one-time cost for each group in the first model cycle. All costs were adjusted to 2023 US dollars using the medical care price index [30].
2.4 UtilityWe calculated QALYs by multiplying LYs by the utility score for each health state. The utility scores, which depict the relative health-related quality of life for an individual in a specific health state, were 0.72 and 0.58 for PF and PD, respectively, obtained from the National Institute for Health and Care Excellence Technology Appraisal 866, guidance for regorafenib for previously treated metastatic colorectal cancer [31]. These utility scores are pooled EQ-5D-3L values collected from CORRECT [8] and CONCUR trials [32], which are phase 3 trials of regorafenib. The CORRECT involved 114 centers in 16 countries in North America, Europe, Asia, and Australia, and the CONCUR involved 25 Asian hospitals in China, Hong Kong, South Korea, Taiwan, and Vietnam. To account for the negative impact of adverse events, we incorporated disutility values for adverse events as a one-off on the basis of a previous cost-effectiveness study of regorafenib [33]. This previous study used disutility values investigated for metastatic breast cancer in the United Kingdom (Table 1) [34]. Due to limited data, we assumed that disutility due to abdominal pain was the equal to the greatest disutility among other adverse events.
2.5 AnalysisThe cost-effectiveness of fruquintinib was evaluated on the basis of the incremental cost-effectiveness ratio (ICER). The ICER was calculated by dividing the incremental costs of the fruquintinib group over the placebo group by the incremental LYs or QALYs. Fruquintinib was considered cost-effective compared with placebo when the ICER was less than US$100,000 per QALY, a commonly used threshold in the cost-effectiveness study [35].
We performed deterministic sensitivity analysis (DSA) and probabilistic sensitivity analysis (PSA) to confirm the robustness of the cost-effectiveness results. The key variables for the sensitivity analyses included drug costs, subsequent treatment costs, follow-up care costs, terminal care costs, adverse event costs, incidence rate of adverse events, utility, and disutility. We adjusted the variables to the lower and upper bounds (± 20%) of their original values in the DSA. For the PSA, we simulated 10,000 times to account for inherent uncertainty and achieve statistically stable results [36]. We used gamma distributions for medical costs and disutility, beta distributions for utility, and normal distributions for the other variables [37]. The standard error was assumed to be 10% for each variable. The sensitivity analyses and simulations were performed using Microsoft Excel (Microsoft, Redmond, WA, USA).
We evaluated the robustness of our results to PFS and OS distributions in scenario analyses by adopting the second best-fitted distributions for PFS (generalized gamma) and OS (log-logistic). Additionally, to understand the influence of utility values on cost-effectiveness outcomes, we performed a scenario analysis incorporating alternative utility sources. Specifically, utility values for PF and PD states of 0.73 and 0.59 were applied on the basis of the CORRECT trial [8].
留言 (0)