
記住我






Malocclusion, a common dental condition, refers to the misalignment of teeth and improper fitting of upper and lower teeth. Among its various classifications, skeletal Class II malocclusion is particularly notable, characterized by a prominent upper jaw or a receding lower jaw. Patients with skeletal Class II malocclusion often present with hyperdivergent facial types. Characteristics of hyperdivergent skeletal Class II malocclusion include the protrusion of the upper jaw and upper lip, incompetent lip growth, poor chin morphology, small nasolabial angles, and an overall long face, which are often the primary concerns for patients.[1,2]
Hyperdivergent skeletal Class II malocclusion has always been challenging to treat in orthodontics due to its characteristics involving both sagittal and vertical dimensions.[3] The key to correcting these inconsistencies is to induce counterclockwise rotation of the mandible, thereby improving the patient’s profile.[4] Conventional treatment of skeletal Class II malocclusion in hyperdivergent patients has primarily involved the extraction of premolars in alleviating dental crowding and improving occlusal relationships. This method creates space, enabling the retraction of anterior teeth and achieving better alignment; however, premolar extraction alone often fails to address the vertical component of the malocclusion adequately.
The conventional approach is often combined with the use of elastics or headgear to manage vertical dimensions, but these methods have limitations.[5] Elastics depend heavily on patient adherence and can introduce unwanted side effects, such as tipping of teeth or increased vertical dimensions. Headgear, while effective in controlling vertical growth, suffers from low patient acceptance due to its bulky and conspicuous features.
In addition, orthodontic appliances such as braces or functional appliances are typically employed in conjunction with premolar extraction to guide tooth movement and improve jaw relationships.[6] However, these appliances primarily influence the sagittal plane and are limited in their ability to exert vertical control. The reliance on patient compliance, particularly with removable appliances, further complicates achieving consistent and predictable results.
Mini-implants (MIs) have emerged as a revolutionary adjunct in orthodontic treatments. MIs transmit forces directly to the jawbone, maintaining the desired tooth position without causing excessive extrusion. Moreover, by providing stable anchorage points, MIs allow for precise tooth movements without relying on patient compliance. MIs have been frequently utilized to regulate the vertical height of the anterior and posterior teeth, thereby causing the mandibles to rotate in a counterclockwise direction and enhancing facial profiles.[7] This technique holds promise for managing vertical facial dimensions in hyperdivergent patients, particularly when combined with premolar extraction.
This research aimed to investigate the effects of MIs on mandibular position and changes in lower face height, as well as their relationship with the position of the maxillary molars and incisors in the camouflage treatment of patients with hyperdivergent skeletal Class II malocclusion. Through a comprehensive analysis, this research can contribute to the optimization of therapeutic strategies, thereby improving the quality of care for patients with complex malocclusions.
MATERIAL AND METHODS Study design and ethicsThis is a retrospective study approved by the Institutional Review Board of 108 Hospital (IRB: 1798/QD-BV). Patients were recruited from the Orthodontic Department at the National Hospital Odonto-Stomatology Hanoi from 2017 to 2021. All subjects provided written informed consent after being thoroughly informed about the study procedure and their rights. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Study subjectsTwenty-seven patients participated in the study, with the age ranging from 15 to 38 years. The sample size was calculated on clincalc.com. Based on a previous study by Costa et al.,[8] anticipated means and standard deviation were entered, the detection power was set at 80%, and the alpha value was set at 5%. Inclusion criteria were (1) hyperdivergent skeletal Class II malocclusion (ANB >3.6°, GoGn-Sn >37°), (2) absence of systemic or chronic conditions, (3) no previous orthodontic treatment, and (4) satisfactory oral hygiene and periodontal health.
ProceduresThe patients received camouflage treatment, which included premolar extraction, retraction of the maxillary incisors, and maximum anchorage using MIs.
Straight wire arch technology was employed to treat all study participants using pre-adjusted MBT appliances with a slot size of 0.022 × 0.028 inches. Treatment began with leveling and aligning using a 0.012-inch nickel-titanium archwire, followed using a 0.019 × 0.025-inch stainless steel (SS) archwire.
MIs (1.6 mm in diameter, 8 mm, and 10 mm in length, Jeil, Korea) were placed bilaterally in the alveolar bone between the maxillary first molar and second premolar. Anterior hooks positioned 2 mm distal to the lateral incisors were installed into the upper arch. Maxillary anterior teeth were retracted using 250 g of force applied through elastic traction from the MIs head to the anterior hooks.
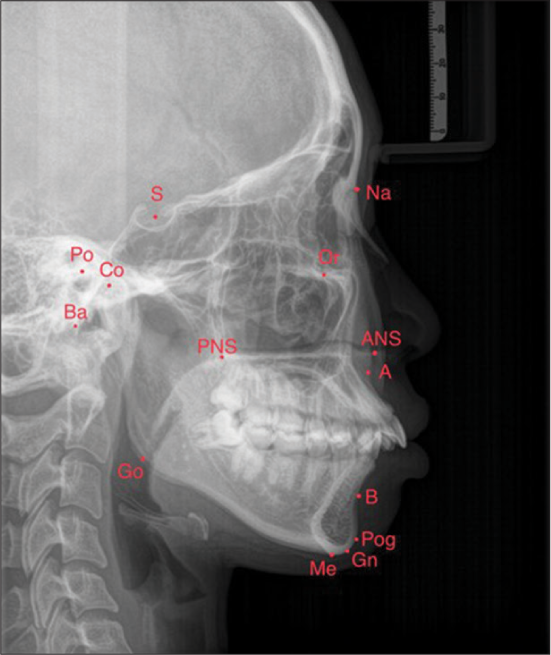
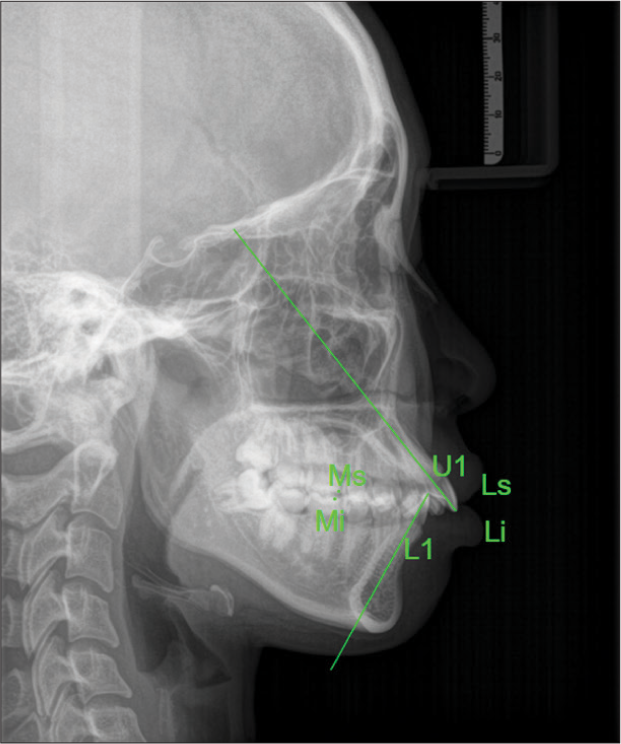
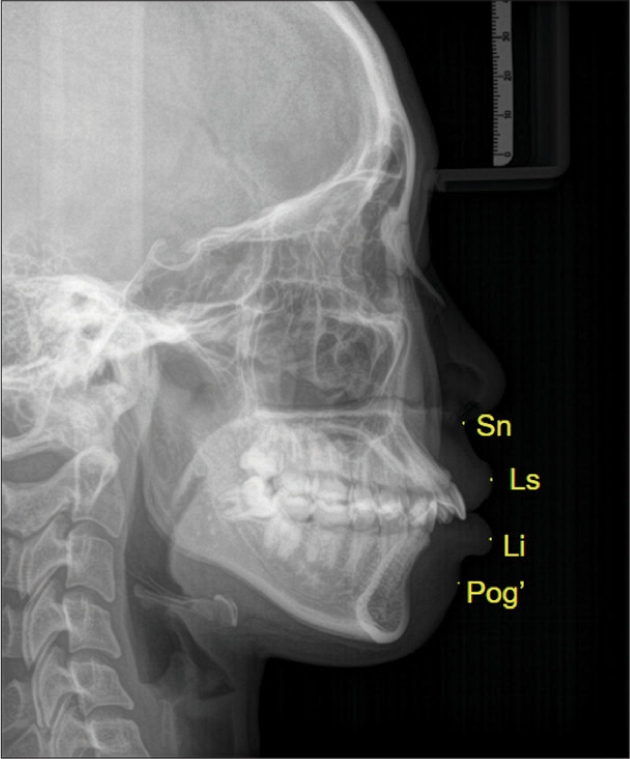
All measurement items were recorded 3 times, and the average value was used as the final measurement result. Cephalometric points, planes was described and explained in [Figures 1-5]. Measurement errors were required to be <0.3° for angles and <0.4 mm for distances. If the error exceeded these thresholds, the reference points were re-evaluated, and the measurements were repeated until they met the required accuracy.
Export to PPT
Export to PPT
Export to PPT
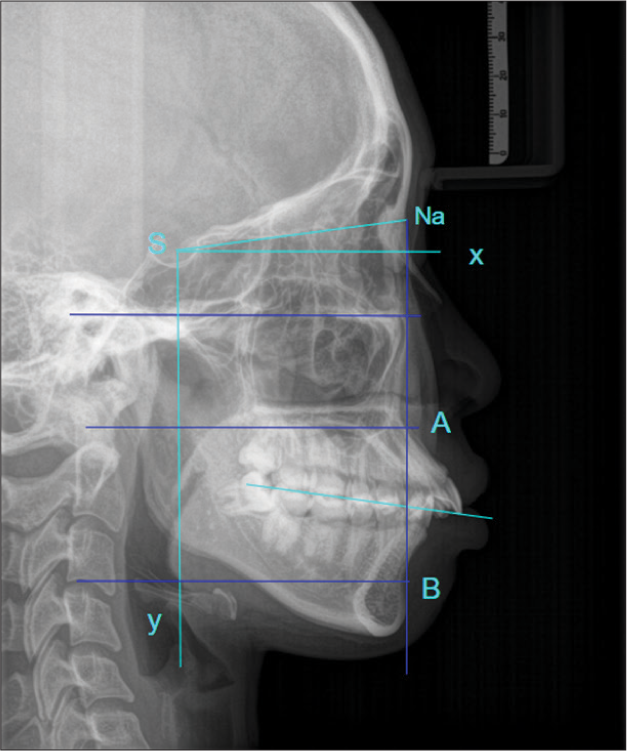
![The Y-axis is defined as perpendicular to the X-axis (forming a 7° angle with the Sella nasion [SN] line downward).](https://apospublications.com/content/9/2024/0/1/img/APOS-92-2024-g004.png)
Export to PPT
Export to PPT
Statistical analysisData were expressed as the mean ± standard deviation. Statistically significant differences were analyzed using the paired t-test. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 22.0 (SPSS® Inc., Chicago, IL, USA). The level of significance was set at P < 0.05.
RESULTSThere was no significant change observed in the SNA and SNB angles (P > 0.05), while the ANS-Me distance showed a significant decrease of −1.98 ± 4.76 mm (P < 0.05). The NBaPtGn angle increased significantly by 1.67° ± 4.08° (P < 0.05), and the Wits appraisal decreased significantly by −0.74 ± 1.45 mm (P < 0.05). The GoGn-SN angle also decreased significantly by −1.05° ± 1.61° (P < 0.05) [Table 1].
Table 1: The cephalometric skeletal variables at T1 and T2 for the hyperdivergent skeletal Class II malocclusion patients (Mean±SD).
Group/Measurements Hyperdivergent P-values Pre-treatmentThe distance from the upper lip to the E-line (Ls-E) significantly decreased by −1.83 ± 2.16 mm (P < 0.05). Conversely, the distance from the lower lip to the E-line (Li-E) significantly increased by −2.61 ± 2.48 mm (P < 0.05). In addition, the distance from the upper lip to the Y-axis (Ls-axis y) decreased by −4.1 ± 5.79 mm, and the distance from the lower lip to the Y-axis (Li-axis y) decreased by −4.52 ± 5.43 mm, both indicating a significant retraction of the lips (P < 0.05) [Table 2].
Table 2: The Cephalometric soft tissue variables at T1 and T2 for the hyperdivergent skeletal Class II malocclusion patients.
Group/Measurements Hyperdivergent P-value Pre-treatmentThe analysis presented in [Table 3] revealed several key insights into the relationships between different skeletal measurements. The first line of [Table 3] showed that GoGnSN significantly influenced ANS-Me (P < 0.05), confirming the suitability of this model. The coefficient for GoGnSN is 0.388, which was statistically significant at the 5% level (P < 0.05), indicating that for every 1-unit increase in GoGnSN, there was a corresponding 0.388-unit increase in ANS-Me. The R2 value for this model was 0.252, meaning that GoGnSN accounts for 25.2% of the variability in ANS-Me.
Table 3: The index of predictable equation correlates between skeletal and soft tissue.
Ending variable Predictable Equation R-square Coefficients regression (a) Constant (b) P ANS-Me 0.252 GoGnSN 0.388*** 23.72*** 0.000 NBa-PtGn 0.047 GoGnSN 0.155* (0.073) 68.84*** 0.073 GoGnSN 0.186 6M-FH 0.842*** 62.813*** 0.000In contrast, the second line of [Table 3] indicated that GoGnSN did not significantly influence NBa-PtGn (P = 0.073), making this model unsuitable for explaining the relationship between these variables.
The third line of [Table 3] demonstrates that 6M-FH had a significant effect on GoGnSN (P > 0.05), validating the use of this model. The coefficient for 6M-FH was 0.842, statistically significant at the 5% level (P < 0.05), indicating that for each 1-unit increase in 6M-FH, GoGnSN increases by 0.842 units. The R2 value for this relationship was 0.186, meaning that 6M-FH explains 18.6% of the variance in GoGnSN.
DISCUSSIONHyperdivergent skeletal Class II malocclusion is particularly challenging to treat in orthodontics due to its sagittal and vertical inconsistencies. These cases often involve skeletal Class II malocclusion with an extremely high mandibular plane angle (GoGnSN >37°), possibly a retrusive mandible, anterior open bite, and severe overjet.
In this study, MI anchorage was used to retract the anterior teeth, extrude the maxillary anterior segments, and intrude the mandibular posterior segments. The results showed that the 6M-FH distance reduced by −1.61 ± 3.74 mm post-treatment, indicating that the first maxillary molar’s distance to the Frankfort plane decreased, and the molar intruded (P < 0.05). The U1-FH distance increased by 1.48 ± 2.11 mm, indicating the first maxillary incisor’s distance to the Frankfort plane increased, and the incisors extruded (P < 0.05). Moreover, the GoGnSN angle reduced by −1.05 ± 1.61°, the ANS-Me distance decreased by −1.98 ± 4.76 mm, and the NBaPtGn angle increased by 1.67 ± 4.08° [Table 1]. These changes suggested the mandible rotated in a counterclockwise direction and the lower face height decreased. The treatment effectively improved the profile both vertically and sagittally.
In treating skeletal Class II malocclusions for patients with a retrognathic mandible and a convex facial profile, orthodontic camouflage can be performed with or without extractions using Class II elastics to coordinate the relationship between the maxilla and mandible.[9] However, Class II elastics and conventional anchorage can generate side effects, including the loss of mandibular anchorage and extrusion of the anterior and posterior teeth. Nanda et al. [10] reported that after 20 years, skeletal anchorage has proven effective in treating open bites and controlling vertical face height, particularly by targeting vertical control of the posterior segments.
Patients aged 15–38 years (mean age 21.7 years) were chosen for this investigation to lessen the impacts of growth. In addition, the upper jaw in the protrusion position was included, and the SNA angle was limited to 80.06 ± 14.59°. Patients with hyperdivergence were included in this study, and the size of the mandibular plane angle was balanced to prevent the measurement results from being affected by differences in mandibular morphologic traits.
Patients with hyperdivergent skeletal Class II malocclusion are typically present with a backwardly rotated mandible rather than maxillary prognathism.[11] In this study, a small but statistically significant level of intrusion was observed for the maxillary incisors (0.1 ± 3.84 mm). The estimated center of resistance for the six anterior teeth is located between the centers of resistance of the four incisors and canines.[12] The applied force had two distinct components: A backward retractive force and an intrusive force. These forces caused bodily intrusion and retraction of the maxillary anterior teeth. From a biomechanical perspective, the types of dental movements, such as root-lingual tipping, crown-lingual tipping, or bodily translation, are ultimately determined by the relationship between the line of action of a force and the position of the center of resistance of a tooth. The occlusogingival position of MIs and the vertical height of the anterior hooks are important factors that can alter the force direction. For instance, using a short anterior hook increases the vertical component and reduces the horizontal component of the force, and vice versa. In this research, with the maxillary MIs located 8–9 mm apical to the bracket slot and the anterior hooks at 2 mm, the force line passed just under the center of resistance. This configuration caused bodily retraction of the anterior teeth with only slight linguoversion.
In this study, the maxillary first molar showed distal movement of 0.1 ± 3.84 mm [Table 4], which was statistically significant. Our findings suggest that the mandible rotated forward. The hinge structure of the temporomandibular complex can explain the relationship between the counterclockwise rotation of the mandible and the reduction in molar and incisor positions (6M-FH, U1-FH) [Table 4]. During the process of retraction using MIs, the intrusive movement of the molars increased the distance between the hinge and the terminal fulcrum, thereby regulating mandibular inclination through the wedge effect. These findings suggest that vertical control of the maxillary incisor and first molar has a fundamental effect on mandibular rotation. The results led to forward and upward movement of the chin, which contributed to the improvement in the facial profile.
Table 4: The Cephalometric teeth variables at T1 and T2 for the hyperdivergent skeletal Class II malocclusion patients.
Group/Measurements Hyperdivergent P-value Pre-treatmentLiu et al.[13] reported that controlling vertical dimensions has always been very difficult in orthodontics. When using conventional anchorage, the extrusion of the maxillary teeth causes the mandible to rotate in a clockwise direction, adversely affecting facial profiles. In the en-masse retraction process, the force line between MIs and the hook intrudes and pulls back the anterior teeth, effectively controlling vertical dimension and improving facial profiles.
Lu et al.[14] reported that MIs made the angle of the mandibular related to the skull plane decrease −1.15° oscillate from −1.67° to −0.63°. In comparison, GoGnSN reduced −1.05 ± 1.61° [Table 1]. In addition, a study of 15 research papers involving 489 patients reported that the first maxillary molar intrusion averaged −1.45 mm, oscillating between −2.02 mm and −0.89 mm (P < 0.001). In our results, the first maxillary molar intrusion was -1.61 ± 3.74 mm with P < 0.05 [Table 4].
According to the predictive equation, when the GoGnSN angle increased by 1 unit, the ANS-Me distance increased by 0.388 units, with a coefficient of R2 = 0.252. This indicated the GoGnSN angle explained 25.2% of the changes in the ANS-Me distance. Similarly, when the 6M-FH distance increased by 1 unit, the GoGnSN angle increased by 0.842 units, with a coefficient of R2 = 0.186, indicating that 6M-FH explained 18.6% of the changes in the GoGnSN angle. The GoGnSN angle’s influenced on the NBa-PtGn angle was not significant (P = 0.073), indicating this model was not suitable for predicting changes in NBaPtGn [Table 3].
CONCLUSIONIn the group with the open mandibular angle and anchored with MIs, the mandible was not rotated downward and backward, the maxillary incisors pulled back more, and the 6th teeth moved forward less than the traditional anchorage group. NBaPtGn facial axial angle decreased compared to before treatment, GoGnSN angle remained unchanged, and ANS-Me lower facial floor height remained the same.
留言 (0)