This study has demonstrated that Māori men who undergo regular PSA testing were less likely to die from PCa compared to Māori men who did not undergo regular testing. Additionally, men who had regular PSA testing were more likely to be diagnosed with PCa but less likely to have a high-grade disease at diagnosis. This may explain the better PCa survival for these men. These findings are consistent with international data on opportunistic and regular PSA screening [3, 6]. The findings of this study are unique, and to our knowledge, this is the only study to assess the “real-world” impact of PSA testing on PCa survival specifically in a Māori population.
In a previous study, we reported that on average, Māori men received 28% fewer PSA tests than non-Māori men over ten years. The same study also showed that Māori men were far less likely to be offered regular PSA tests across all age groups as part of an opportunistic PCa risk assessment [7]. Furthermore, our group has previously concluded that PCa-specific survival in NZ is significantly lower for Māori men compared to non-Māori [7, 8]. We reported that the 10-year CSS for Māori was 71.5% compared to 79.3% for Europeans, 83.9% for Asians and 76.3% for Pacific Island men. This corresponded to a 44% higher risk of PCa death for Māori men compared to Europeans [8].
The current study has shown a strong association between the rate of PSA testing and PCa-specific survival with men in the non-SG at least twice as likely to die from PCa compared to the ScG. One of the strengths of this study is that only Māori men were included. This has minimised potential confounding factors which might impact PSA testing, diagnosis and survival. These factors include cultural barriers to PSA testing, and treatment-related factors [4, 7].
PSA screening has been shown to improve PCa-specific survival in large randomised studies, and the relationship between PSA testing and PCa survival is not a new finding [3]. The ERSPC clearly showed a survival advantage at 16 years of follow-up. Additionally, analysis of the same study has demonstrated that within the study population, socioeconomic factors seem to impact the rate of PSA testing, subsequent PCa diagnosis and PCa survival [9, 10]. Our study confirms that these findings apply to the NZ population.
Men in the non-SG were younger (54 vs. 51 years). Therefore, they may not have been eligible for regular testing since most practitioners start to offer testing to men in their 50s. However, it should be noted that the ScG had a median of three cycles of testing, which suggests that the three-year median difference in the age of the groups does not explain the significant variation in testing. Also, a larger proportion of the non-SG died of PCa, indicating that testing in Māori men effectively reduces PCa mortality. Therefore, PSA testing should perhaps start at an earlier age in Māori.
We found the increasing NZDep index was associated with a slight reduction in PCa diagnosis. This aligns with other prior studies which suggests socioeconomic status has an impact on PSA testing regardless of ethnicity [4, 7].
Another important consideration in our study was the definition of regular PSA testing. It is accepted that only recurrent PSA testing at regular intervals results in improved PCa outcomes and that low-intensity and infrequent testing has no positive impact on the outcomes [11, 12]. Men in the ScG had a median of three tests during the 12-year study period, which fell well within the accepted definitions for PSA screening. Pakarainen et al. reported that in the Finnish arm of the ERSPC trial, men who attended two or three rounds of screening experienced improved PCa survival [11].
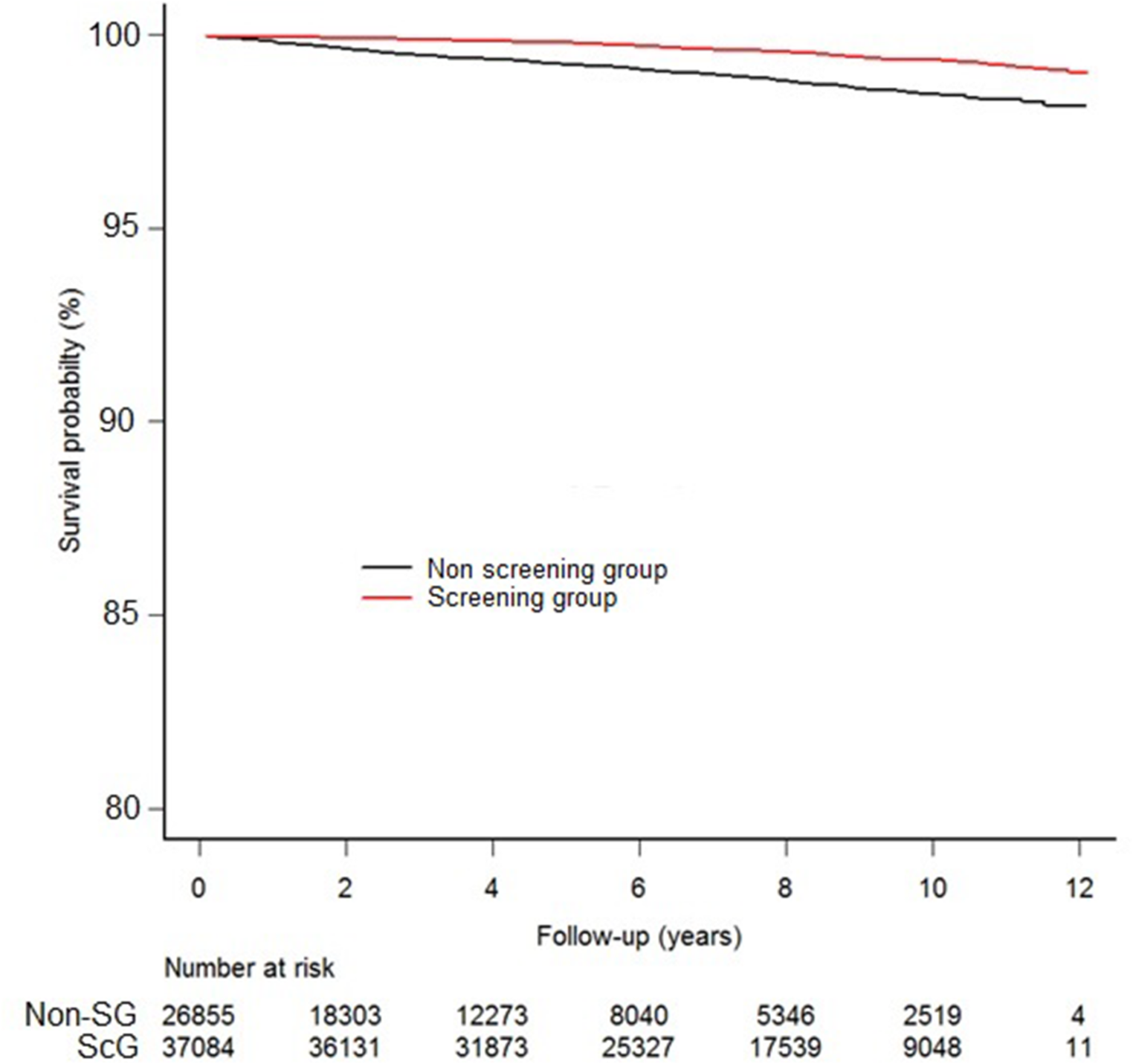
The CSS was significantly lower in the non-SG. This indicates that in real-world settings, regular PSA testing significantly impacts PCa survival in Māori men. Our study suggests that the previously reported disparities in PCa outcomes in Māori compared to non-Māori may be addressed by ensuring equitable access to regular PSA testing for Māori [13]. As seen in Fig. 1, most PCa deaths in the non-ScG occurred within six years following diagnosis, inferring that this was primarily death from aggressive high-risk disease. The discrepancy in median follow-up time between the non-SG and ScG was an interesting finding. Men in the non-SG may have fewer PSA tests because of reduced engagement with health care services or competing comorbidities leading earlier to loss to follow-up. However, we cannot comment with certainty the reason for this due to the retrospective nature of our study.
Our study has also demonstrated that regular PSA testing was associated with an increased risk of PCa diagnosis. This aligns with international studies and represents the well-established potential harm of overdiagnosis in PCa screening [14, 15]. However, the difference in the rates of low-risk disease between the ScG and non-SG groups was merely 7.7%. With advancements in cancer detection and the broader applicability of active surveillance, the balance in this cohort may well be leaning toward the survival benefits achieved through regular PSA testing [16].
Our study has some limitations. Firstly, the study is a retrospective analysis of prospectively collected data. We cannot ascertain if the two groups were identified as no data on comorbidities was available in the dataset. The baseline PSA level between the two groups was not compared. However, all men in this cohort had a PSA test and therefore were deemed “fit enough” for PCa screening by their primary healthcare providers. Secondly, there were no data on PCa disease stage at diagnosis, the treatment received or the length of follow-up between the study groups, which could impact patient outcomes. This information was generally poorly documented in the NZCR for PCa. In addition, our study did not identify causes for the different rates of PSA testing among Māori men. However, despite these limitations, we found significant differences in the outcomes.



留言 (0)