Study design
After institutional board review approval (CNIL number: 2234449v0), the data of all female and male patients who underwent a robotic AUS implantation at a single academic center between January 2010 and December 2022 were collected prospectively (female patients) or retrospectively (male patients). All the implantations were performed by three surgeons in their learning curves over the study period. The database was analyzed retrospectively for the purpose of the present study.
Prior AUS implantation and neurogenic SUI were the only exclusion criteria. The following baseline characteristics were recorded in a dedicated computerized dataset for all patients: age at the time of AUS implantation, body mass index (BMI), ASA score, etiology of incontinence (neurogenic vs. non-neurogenic), history of radiotherapy, history of previous anti-incontinence surgery, number of pads per day, type of pad, presence of urgency, maximum free urinary flow (Qmax), post-void residual volume (PVR). All patients had to fill out the International Consultation on Incontinence Questionnaire – Short Form (ICIQ-SF) and Urinary Symptom Profile questionnaire (USP) prior to surgery and at any follow-up clinics as part of the institution’s routine practice. Unlike for female implantations, male patients did not have a systematic urodynamic assessment prior to surgery.
Patient’s selection
For male patient, AUS was offered as an option to all patients presenting a positive cough stress test.
AUS was offered to all female patients with SUI due to ISD defined as a positive cough stress test with a poorly mobile or fixed urethra on physical examination. Urodynamic was performed in all of these female patients and a low maximum urethral closure pressure (MUP) was deemed as a co argument of ISD.
AUS implantation and activation
All female AUS were implanted using an anterior transperitoneal robot assisted approach according to the technique previously described [7] except for two implanted using a preperitoneal robot-assisted approach. The sphincter cuff was placed around the bladder neck in all cases.
For male AUS, the sphincter cuff was placed around the bulbar urethra. The surgical approach was either perineal or penoscrotal depending on the surgeon’s preference.
The urethral catheter was removed in the operative room or on day 1 postoperatively, except in cases of bladder injury where it was kept for 10 to 14 days. The AUS was activated at six weeks for all patients and then the patient was seen at 3 months and then yearly and in case of any intercurrent event.
Outcomes of interest
The primary endpoint of the present study was the continence status at 3 months categorized as: complete resolution of SUI (0 pad), improved SUI (1 pad a day) or unchanged SUI (> 1 pad a day).
The secondary endpoints were (I) continence status at last follow-up (II) post-operative complications (III) major postoperative complications defined as a Clavien Dindo Grade of 3 or higher (IV) explantation free survival of the device (V) revision free survival of the device (VI) Other perioperative outcomes: mean operative time, estimated blood loss, cuff size, length of hospital stay.
The postoperative complications were recorded and graded using the Clavien-Dindo classification [8].
The last follow-up was defined as the most recent date on which information was gathered, either during an outpatient clinic or by phone call to update the patient’s data.
Explantation was performed when cuff or pump erosion occurred or in cases of device infection. It was also offered in rare cases for difficulties in manipulating the pump that remained unsolved despite repeat hospitalizations for patients’ education. A revision of the device was performed for mechanical or non-mechanical failure. In rare occasions, it was used to relocate the pump after difficulties manipulating it or because of pain in seated-position.
Statistical analysis
Means and standard deviations were reported for continuous variables, medians and ranges for categorical variables, and proportions for nominal variables. Comparisons between groups were performed using the χ2 test or Fisher’s exact test for discrete variables, and the Mann-Whitney test for continuous variables as appropriate.
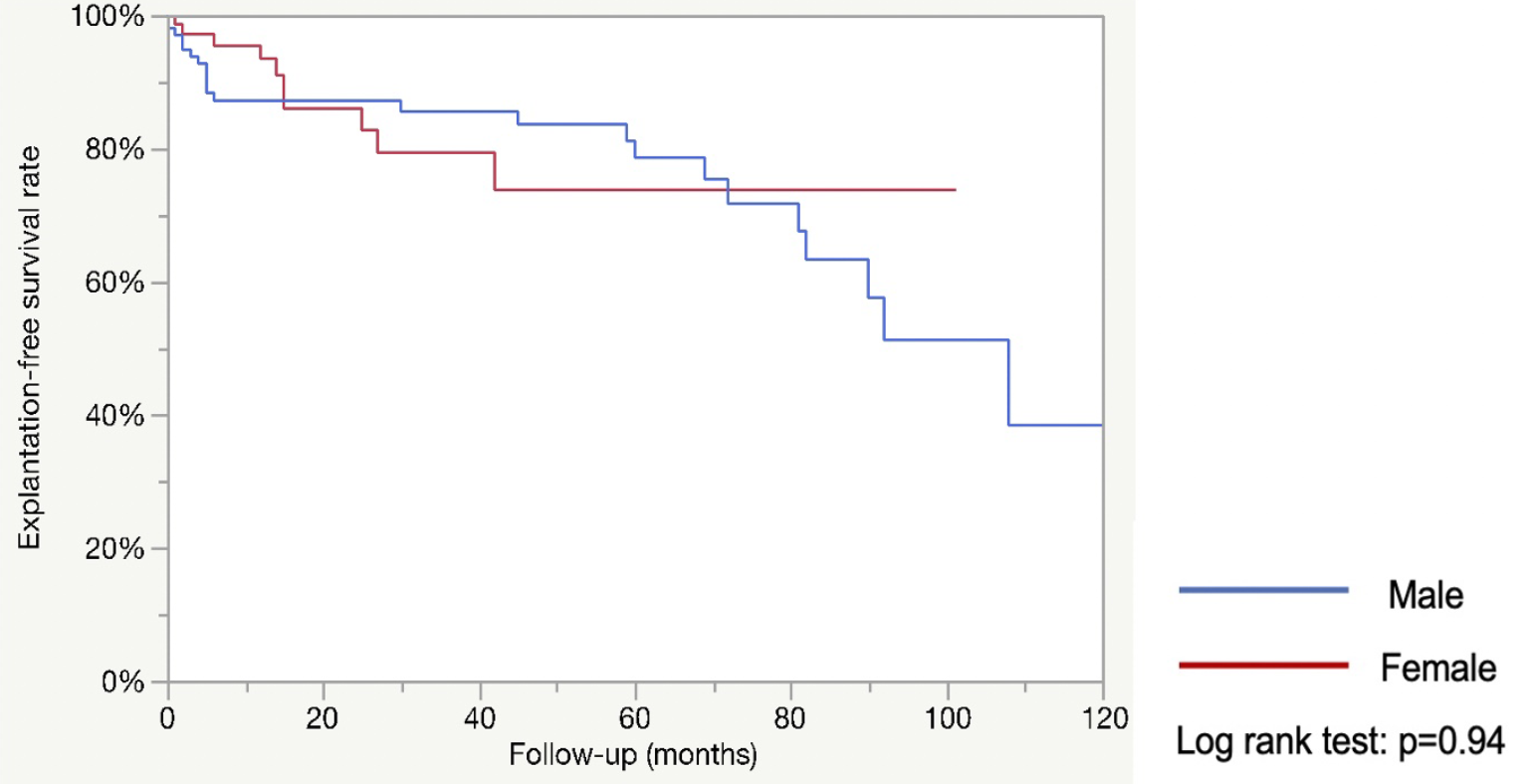
We performed multivariate logistic regression analysis to assess the predictive factors of continence at the last follow up. The probabilities of revision-free and explantation-free survivals were estimated using the Kaplan-Meier method.
Patients without any event (revision or explantation) during the study period were censored at the date of the last follow-up. Statistical analyses were performed using JMP v.12.0 software (SAS Institute Inc., Cary, NC, USA).
All tests were two-sided with p < 0.05 as a threshold to define statistical significance.



留言 (0)