Significantly higher proportion of patients opted for early ureteroscopy as the treatment of choice over a trial of MET. Early URSL has better results in terms of patient centred outcomes. It is associated with better satisfaction rate due to early definitive treatment of stone, high stone clearance rates and less anxiety related to fear of recurrent colic episodes and stone related complications.
After SDM, URSL was the preferred treatment over MET, reflecting literature that links treatment choices to more successful outcome [16]. The invasiveness of URSL did cause more decisional conflict, yet its higher selection rate suggests a patient bias towards avoiding the recurrence of pain and frequent emergency hospital visits over the risks of an invasive procedure. The correlation between larger stone sizes and the choice of URSL likely points to the communicated lower efficacy of MET for larger stones during SDM sessions.
Decisional conflict denotes the uncertainty patients feel when making tough healthcare choices. In our study, those opting for URSL faced greater difficulty deciding, possibly due to the procedure’s invasiveness, associated risks, anaesthesia concerns, and recovery duration. The precise causes of this increased decisional conflict remain unexplored, highlighting a need for further research into these specific factors (Table 1).
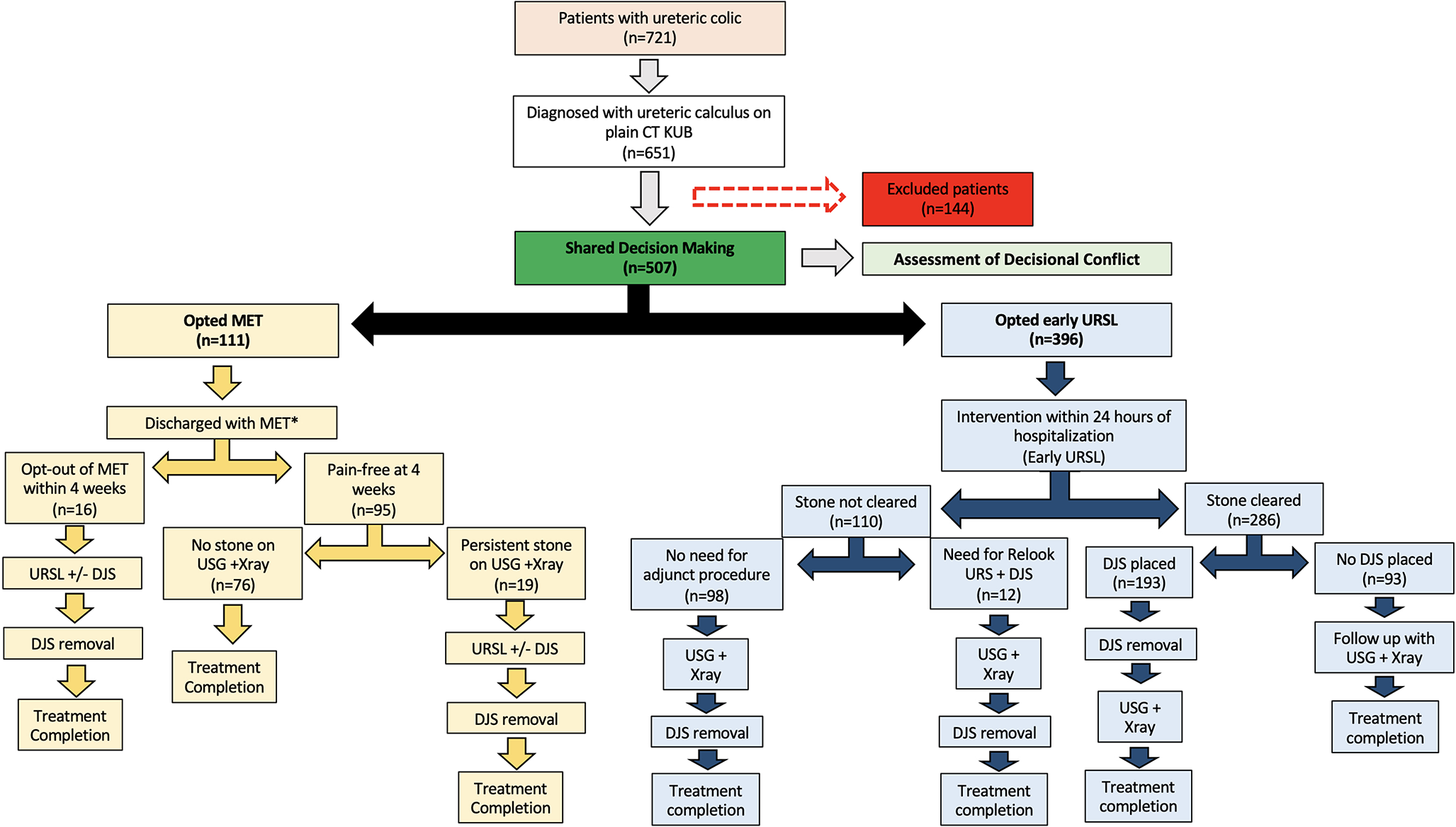
In our study, we mirrored a real-world clinical scenario by allowing patients with ureteric colic to choose between early URSL and MET, facilitating a more natural SDM process. We determined treatment success by the absence of further treatment interventions, thereby minimizing unnecessary radiation from repeat CT scan. Using this strategy, the likelihood of overlooking asymptomatic residual stones was considered to be minimal [17]. In the URSL group, fragments of size 2 mm or less were considered clinically insignificant as they pose minimal risk of recurrent colic or complications [18]. The study’s pragmatic design enhances the applicability of the results by comparing the two treatment modalities in practical scenarios, unlike RCTs that operate under more controlled but less real-world conditions.
CUSP-Questionnaire responses indicated that MET patients experienced higher pain and anxiety, mainly due to uncertainty over outcome, implying a potentially larger psychological impact compared to those who chose early URSL. Conversely, URSL patients reported more disruption to work and daily life, underscoring the importance of considering lifestyle impacts in treatment decisions (Table I). The increased disruption to work and daily life in the URSL group could be attributed to the self-imposed restriction and leave from work in URSL patients due to the influence of the operative procedure, despite early discharge and encouragement for early return to normal activities following the procedure.
Subgroup analysis of stones ≤ 5 mm revealed that URSL patients had significantly lower decisional regret, suggesting greater satisfaction with this choice. For stones > 5 mm, the MET group’s regret scores were notably higher, indicating more dissatisfaction likely due to the non-invasive approach’s failure to quickly resolve symptoms, exacerbating regret when additional interventions became necessary. These comprehensions suggest that patients who are particularly anxious or concerned about the potential need for additional treatments, risk of recurrent colic or the protracted duration of treatment required for achieving stone clearance, may be better served by early URSL. Clinicians should recognize the potential for decisional conflict and regret and address them using decision aids and comprehensive shared decision-making strategies [19].
This study has several strengths, including its large sample size and the use of validated measures to assess decisional conflict and patient-reported outcomes. When multiple treatment modalities with equally or nearly equivalent outcomes are available, patient perspectives play a major role in making an informed decision for the selection of treatment. While the impact of treatment choice on patient outcomes, such as treatment regret and health-related quality of life, is well established for prostate cancer [20, 21], its effects on patients with ureteric stones are less understood. A patient who comprehends the logic of treatment and follow-up is more prepared to translate treatment plans into a workable daily routine of disease management [22]. With the development of a variety of more efficacious treatment approaches, the clinical emphasis on assessing patient’s preferences and discussing different treatment options has become increasingly important [22]. The benefits of increased patient participation in treatment plans have already been demonstrated in literature [23, 24]. Previous studies have reported patient outcomes with self-selected therapy for ureteral stones, but have not evaluated why patients make decisions with regards to which treatment approach is best for them [25]. This study provides an innovative insight into patient-centric outcomes during ureteric colic treatment in real-world settings. Its findings have the potential to improve patient decision aids for ureteric stone treatment by offering crucial patient-centric data, thereby assisting future patients in making well-informed decisions.
Our study’s limitations include its reliance on questionnaires and the lack of data on employment, insurance, and income, which could influence patient decision-making. The sole recruitment from a University Teaching Hospital may not reflect the broader population, particularly first-time stone formers, due to participants’ potential prior stone experiences and interventions. Additionally, follow-up evaluations of MET patients used USG or X-ray instead of CT, reducing radiation exposure but possibly overlooking some asymptomatic retained stones. Exclusion of patients opting for ESWL in an attempt to provide direct comparison between two treatment modalities can also be considered as another limitation of the study.



留言 (0)