"Swiss Cheese" VSDs represent the most critical subtype among muscular VSDs. This subtype exhibits elevated mortality rates, an increased risk of residual shunt and reoperation, as well as heightened susceptibility to ventricular dysfunction and heart block when contrasted with isolated perimembranous defects [14]. Surgical intervention for "Swiss Cheese" VSDs presents a formidable challenge, especially when confronted in neonates and premature infants with low body weight. Currently, there is no consensus regarding the optimal management of "Swiss Cheese" VSDs. Conventional surgical repair for "Swiss Cheese" VSDs yields unsatisfactory outcomes, primarily due to significant intraoperative challenges arising from the obscured boundaries of defects by the moderator band and multiple trabeculations. Closing apparent defects may reveal additional hidden defects, necessitating further intervention [14, 15]. Therefore, in the past several decades, various strategies have been described, including device closure, re-endocardialization of the interventricular septum, PAB, as well as diverse surgical approaches and techniques [5, 11, 16].
One classic technique involves repairing all VSDs using a single large autologous pericardial patch, polytetrafluoroethylene patch, or a composite patch composed of Dacron lined with preserved heterologous pericardium [6,7,8, 17]. This approach has demonstrated satisfactory short- and mid-term outcomes, with specific advantages highlighted in the repair of apex trabecular VSDs [14]. However, it is important to note that an oversized patch may impede the movement of the ventricular septum and limit the development of the right ventricle, potentially leading to late diastolic dysfunction and subsequent complications such as right heart failure, cardiac cirrhosis, and atrial tachyarrhythmias [18, 19]. Brizard et al. [20] introduced a novel approach incorporating intraoperative echocardiography and the utilization of double patches to sandwich the septum. Nevertheless, replicating this technique poses significant challenges, and it has not consistently produced satisfactory outcomes. In their cohort, failure to localize all defects resulted in PAB in two patients, while two other patients required permanent pacemaker insertion. Sakurai et al. [11] reported the successful application of a novel technique for repairing 'Swiss Cheese' ventricular septal defects in a single case, using a combination sandwich patch composed of three polytetrafluoroethylene patches. However, to date, no further studies have been published on this technique.
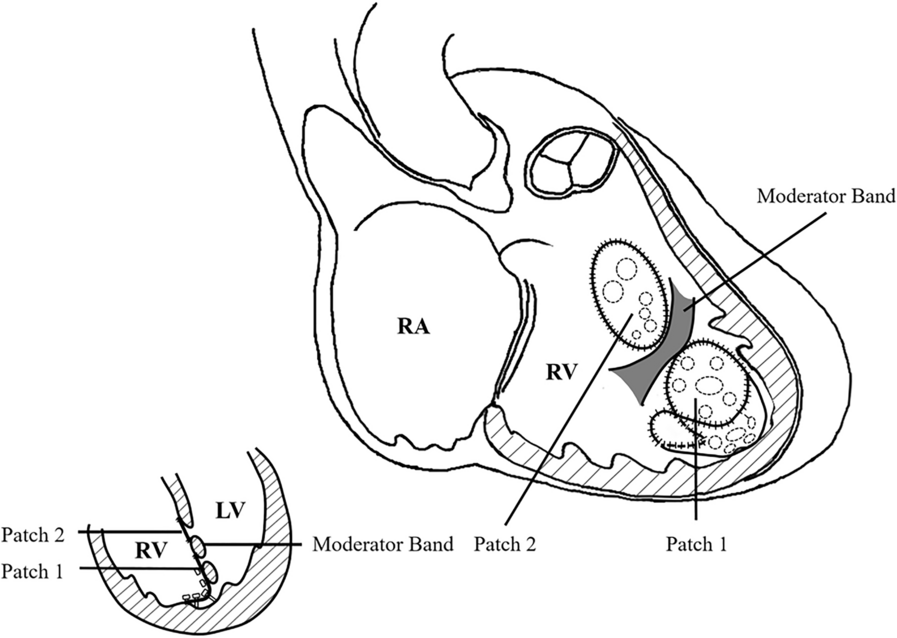
Since 2014, we have adopted a modified procedure for "Swiss Cheese" VSDs to mitigate the potential drawbacks associated with the "single oversized patch" technique. This approach includes the repair of outflow tract VSDs with one glutaraldehyde-treated or fresh autologous pericardial patch, as well as the repair of apex trabecular VSDs and exclusion of the RVA with another fresh autologous pericardial patch. Mid-term follow-up results were favorable, with no significant complications observed during a median follow-up period of 4.9 years (range: 2–9 years). TTE and CMR revealed satisfactory left and right ventricular systolic and diastolic function, with no discernible reduction in right ventricular volume and no evidence of thrombosis. These findings suggest that the employed technique is safe and may have a lesser impact on the movement of the ventricular septum and fewer constraints on the development of the right ventricle compared to the "single oversized patch" technique.
During the procedure, a Foley balloon catheter can be employed to enhance exposure of the VSDs, as detailed in the preceding procedural section. This approach offers potential advantages in delineating the extent of VSDs and mitigating residual shunting post-operation. The exclusion of the RVA is pivotal to preventing residual shunt. Geva et al. [21] demonstrated that the right ventricular inlet (or right ventricular sinus) constitutes 81 ± 6% of the combined right ventricular end-diastolic volume and 87 ± 4% of the combined stroke volume. Therefore, exclusion of the RVA may not significantly influence the right ventricular end-diastolic volume.
For patching, especially in cases involving apex trabecular VSDs, the use of fresh autologous pericardium is recommended due to its reported favorable biological characteristics, including freedom from retraction, stiffness, fibrosis, and calcification [22]. Consequently, it is less likely to adversely impact right ventricular function in the mid- or long-term. During the patching phase, it is advisable to position the suture of the anterior wall of the right ventricle as close as possible to the RVA. Additionally, excising small trabeculae is recommended, and interrupted pledgeted sutures should be strategically placed between the patch and trabecular muscles for intermediate fixation to prevent septal bulging. These maneuvers minimize the volume of the right ventricular cavity separated into the left cardiac system, thereby effectively preventing excessive reduction of the right ventricular cavity and postoperative ventricular dysfunction.
The two-patch and RVA exclusion technique is primarily intended for patients older than 3 months with "Swiss cheese" VSDs, particularly those with muscular VSDs located near the apex. In infants under 2–3 months requiring ventilator support, especially those with complex defects, delicate heart muscles and limited exposure during surgery may negatively impact outcomes of this technique. Therefore, preemptive PAB is recommended to safeguard the pulmonary vascular bed and alleviate symptoms of congestive heart failure [5]. Subsequent definitive repair is typically advised within 3–6 months.
The primary concern centers on the persistent impairment of right heart diastolic function due to the exclusion of the RVA. Additionally, heart block stands out as a potential late complication resulting from the extensive intracardiac sutures. Consequently, patients necessitate continued long-term monitoring, involving regular ECG, TTE, and especially CMR to evaluate right heart functionality.






留言 (0)