
記住我





This case study describes a 60-year-old female, smoker, with a history of permanent pacemaker (PPM) implantation 8 years prior to presentation. She presented after undergoing a routine checkup as a part of her work policy which showed evidence of atrial fibrillation (A-fib) on electrocardiography (ECG). The patient described a history of intermittent dizziness, which spiked and self-terminated. She had a history of PPM implantation done 8 years ago which was done for her after she complained of dizziness and a holter monitor done for her which showed significant pauses. Pacemaker switched off two years ago after implantation when her checkup showed that the patient rarely used in past years. She had a longstanding smoking history. No history of cardiac illness or any other malignancies in her family. On physical examination, the patient was vitally stable, afebrile. Blood pressure within normal limits. Heart rate was 77 beats per minute, temperature 36 degrees Celsius, respiratory rate of 20 beats per minute, oxygen saturation 96% on room air, blood pressure 116/86 mmHg. ECG showed episodes of ventricular tachycardia.
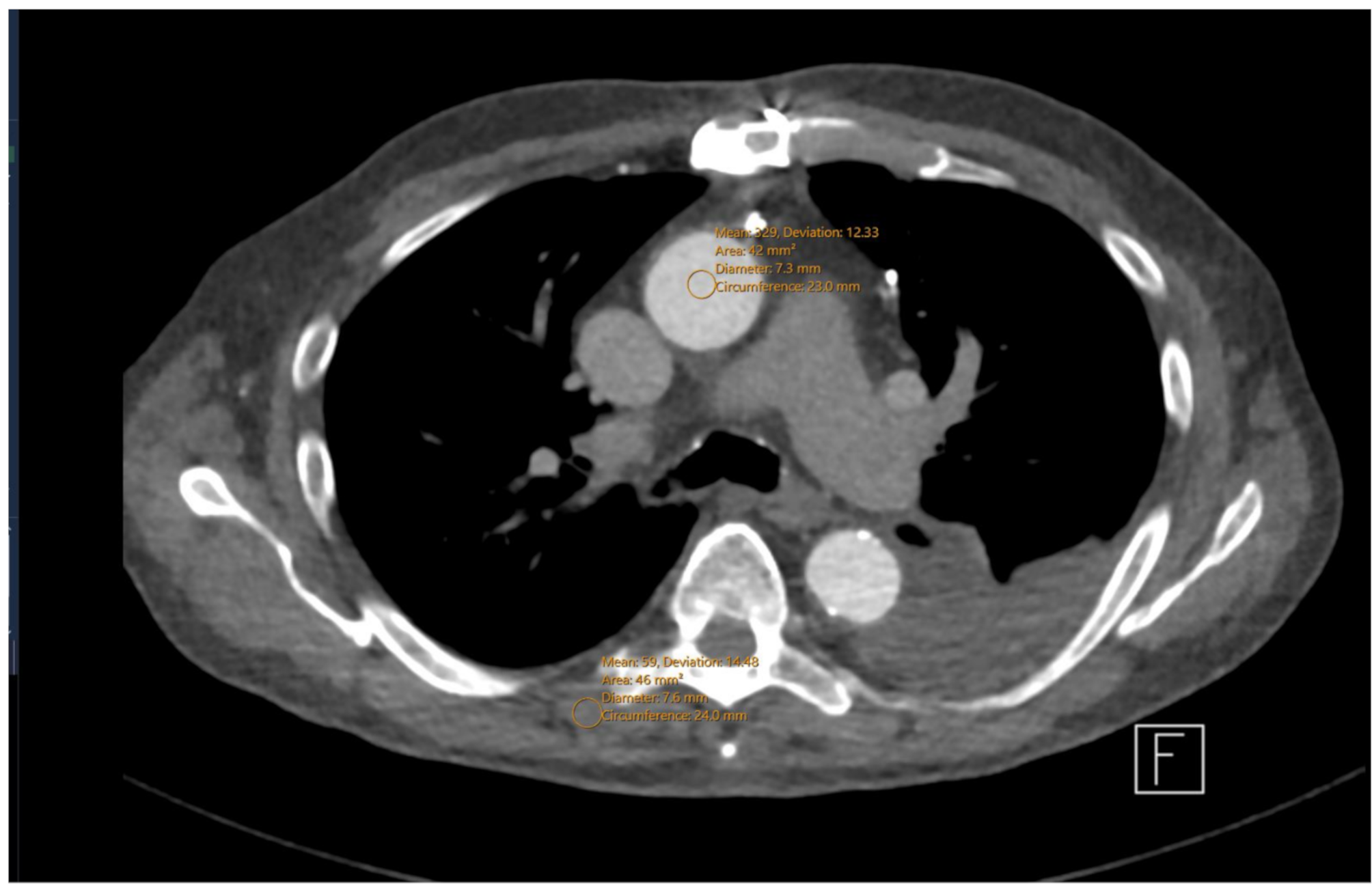
Her present echocardiogram showed a large pedunculated mass, not mobile, oval shape with smooth margins, attached to the apex and occupying most of the left ventricle cavity. The mass is obliterating the left ventricular outflow tract (LVOT) and interfere with mitral valve function. Sever left ventricular systolic dysfunction (LVSD) noted with left ventricular ejection fraction (LVEF) 20%. The left atrium and right atrium appeared of normal size and function, with intact interatrial septum and no evidence for an arterial septal defect. The mitral valve was normal in structure and function with no evidence of stenosis or prolapse. All other valves are normal in function and structure. No evidence of pericardial effusion. The right ventricle was normal in size and function, normal wall thickening, and normal right ventricular systolic function. Cardiac catheterization showed normal coronary arteries. A computed tomography (CT) scan revealed a lobulated well-defined hypodense mass occupying the left ventricle, measuring 5 × 4.3 × 4 cm (Fig. 1A). Cardiac magnetic resonance imaging (MRI) confirmed the presence a left ventricular mass. No pericardial or pleural effusion, consolidation, pulmonary nodules. No evidence of intrathoracic or intraabdominal masses found, and normal cerebral vasculature noted. The patient admitted for left ventricular mass excision through ventriculotomy. The patient brought to the operating room, intubated under general anesthesia and lined up. She prepped and draped in supine position with sterile fashion. Median sternotomy with pericardiotomy done. Aorta and right atrial cannulation done. The patient was on cardiopulmonary bypass. Vent and cardioplegia cannula were inserted in the aorta and aorta was crossclamped and cardioplegia delivered. Through left ventriculotomy incision, the mass was adherent to the ventricular wall and was easily dissected with left ventricular incision repair. Frozen section consultation showed a spindle cell tumor favoring muscular origin. Complete surgical resection was performed with no complications. The patient tolerated the procedure well and was transferred to cardiac surgery intensive care unit (ICU) in stable condition with good hemodynamics. The specimen was sent for histopathology analysis. Gross pathological examination of the specimen revealed a firm, oval, well-circumscribed mass with a smooth outer surface, measuring 6 × 4.5 × 2.5 cm (Fig. 1B). Histopathology examination revealed well-delineated benign neoplastic tissue composed of interlacing bundles of smooth muscle cells separated by a small amount of connective tissue (Fig. 1C). These cells were elongated cigar-shaped spindle cells with fibrillary acidophilic cytoplasm, characteristic of leiomyoma (Fig. 1D). There was a small focal area of degenerative nuclear atypia changes. However, there was no evidence of increased mitotic activity [less than 1/ 10 high power field (HPF)]. No evidence of necrosis or hyper cellularity were seen. Tumor cells were positive for desmin, smooth muscle actin (SMA) (Fig. 1E), muscle-specific antigen (MSA), and H-Caldesmon (Fig. 1F). Estrogen (ER) and progesterone receptors (PR) showed faint nuclear staining. They were negative for myogenin and myoglobin. Overall, the patient’s histology and immunohistochemistry results were diagnostic of leiomyoma.
Fig. 1Radiology, representative hematoxylin and eosin (H&E) and immunohistochemical staining of cardiac leiomyoma. (A): Computed Tomography (CT) scan with contrast of the chest revealed lobulated well-defined hypodense mass occupying the left ventricle measures 5 cm. no evidence of intrathoracic metastasis. (B): Gross examination of a well circumscribed mass containing white-tan whorled cut surface. No areas of necrosis are seen. (C): Sharply demarcated neoplastic cells composed of smooth muscle bundles proliferation, arranged in whorled pattern. No mitosis, necrosis, nor atypia seen (H&E; 4x). (D): Tumor cells are composed of spindle cells with classical cigar-shaped nuclei, interlacing fascicles (H&E; 20x). (E): Tumor cells expressing strong SMA staining (10x). (F): Tumor cells expressing strong H-caldesmon staining (10x)
Postoperative echocardiogram showed left ventricular systolic function moderate to severe impairment with ejection fraction of 30 to 35. No evidence of left ventricular mass. No pericardial effusion. Her laboratory investigation of White Blood Count (WBC) 11.7, Hemoglobin 13.1, Platelet 333, Sodium 143, Potassium 4.6, Urea 7.4, Creatinine 83, Estimated glomerular filtration rate (EGFR) more than 60. On physical examination, chest is clear on auscultation bilateral, no added sound. Cardiovascular (CVS) examination, S1, S2 plus 0. Abdomen was soft and lax, nontender, no organomegaly. Extremity good peripheral pulses. No lower limb edema. Central nervous system (CNS) examination sensory and motor examination grossly intact. Patient followed up in the outpatient clinic, her wound was clean, and she looked healthy. Four-year follow up, the patient is healthy and doing well with no disease recurrence.
留言 (0)