We present two cases of paracardiac tumors involving a CAS (case 1) and an IgG4-RD (case 2), with the latter being the sole manifestation of the disease. Despite utilizing a multimodal imaging approach, and given the complexity of the cases, a multidisciplinary team planned the surgical procedures utilizing 3D models. The 3D models provided extensive information about the margins between the masses and cardiac tissue, aiding in directed treatment in case 1 and resection in case 2.
Cardiac tumors are rarely encountered in day-to-day cardiology practice, with an incidence of 1,380 per 100 million individuals [12]. Tumors can be categorized as either neoplastic or non-neoplastic. Among neoplastic tumors, secondary tumors or metastases are significantly more common, being up to 132 times more frequent than primary tumors [8]. Furthermore, primary cardiac tumors are predominantly benign (90%), with only a small proportion being malignant (10%) [13, 14].
The approach requires a multimodal imaging evaluation, including echocardiography, CCTA, and CMR. However, a biopsy is mandatory for proper diagnosis chambers and to the right coronary artery, due to its habitual location, resection is often impossible [15]. Therefore and treatment in many cases, especially in suspected malignant lesions, with complete surgical resection recommended in certain cases. Alongside CMR, CCTA presents a favorable diagnostic option for identifying calcified masses and examining thoracic morphology and associated vascular structures [6]. The clinical approach requires a multimodal imaging evaluation, including echocardiography, CCTA, and CMR, although in some cases more is needed, and the use of new technologies is required [7].
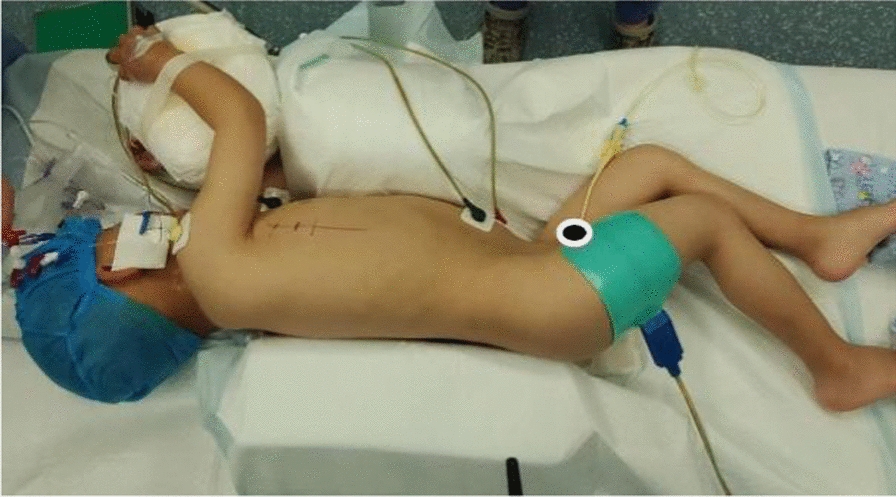
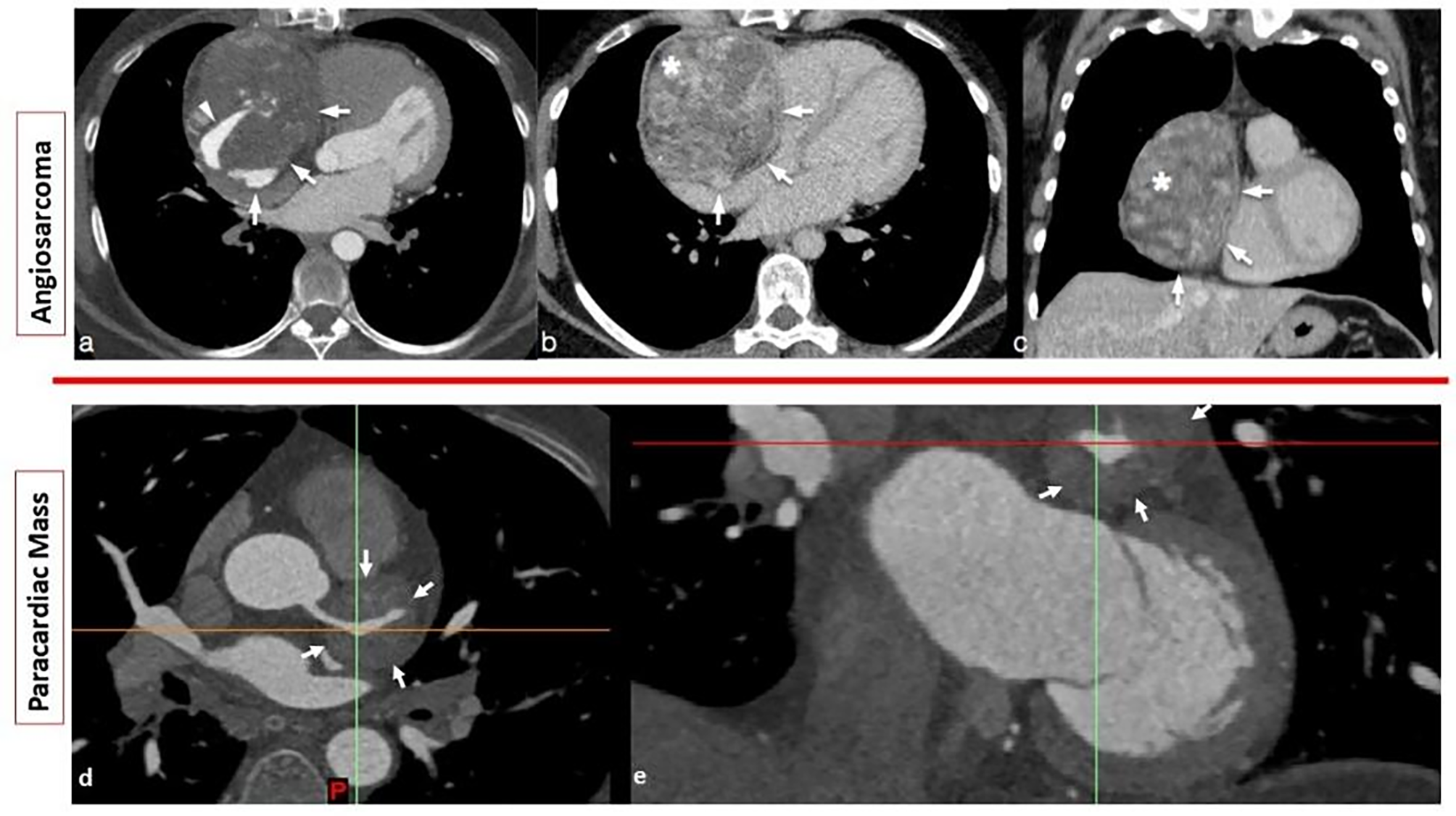
Cardiac sarcomas, particularly cardiac angiosarcomas (CAS), constitute the majority of primary malignant tumors of the heart, with around 40% of cases reported in case series [9, 10]. They are typically located at the right atrium in 75% of cases [7]. Surgical resection confers the best long-term outcomes; however, considering the high likelihood of metastasis at presentation and infiltration to right sided chambers and to the right coronary artery, due to its habitual location, resection is often impossible [15]. Therefore, neoadjuvant chemotherapy with debulking may often be the treatment of choice. For case 1, macroscopic evaluation confirmed the 3D model findings. It allowed the surgical to approach a sequential surgical resection with partial tumor excision aided with neoadjuvant chemotherapy, this due to the evidence of large size and extent of the tumor infiltrating the right ventricular free wall, in which a complete excision in the first attempt was deemed impossible without safely preserving vital structures (Fig. 5a) with a high risk of vascular complications and ventricle laceration. At follow-up, one year after therapy, it was decided to resect the tumor and 18 months later the patient has no local recurrence or related symptoms.
IgG4-RD is known to cause fibroinflammatory lesions in nearly any organ system. However, diagnostic criteria established by the American and European League Against Rheumatism do not include cardiac involvement as a criterion its diagnosis [11]. Cardiac manifestations can vary widely, including pericarditis, myocarditis, valvular heart disease, cardiac masses, and coronary involvement [16]. Early recognition of cardiac manifestations is crucial for initiating directed management and treatment, potentially reducing disease extension, as cardiac involvement may precede systemic manifestations when detected early [17]. Coronary involvement, characterized by the “mistletoe sign,” is reported in up to 15.4% of cases and can present with coronary stenosis or aneurysms in 65% and 40% of cases, respectively, often leading to symptomatic presentations such as coronary syndromes [16]. The “mistletoe sign” is characterized by a perivascular mass surrounding the coronary artery (See Fig. 4), resembling the mistletoe plant attached to the three branches, albeit rare its clinical utility lies that it serves as a characteristic of IgG4-RD, and therefore aid diagnosis of this rare condition directing treatment [18]. Moreover, it might serve as a follow-up marker as reports have shown remission of this sign with directed treatment [18].
In case 2, the mass was found to be incidental, with no involvement of other organs, despite extensive evaluation. Considering its broad differential diagnosis and close relationship to vital structures, we generated a 3D model in printed and digital forms to corroborate the surgical approach. A 3D-printed model was created, separating the vital structures with the mass cut in half to demonstrate LMCA involvement; this approach helps to show the typical “mistletoe sign” coronary involvement as shown in Fig. 2. Finally, a dynamic simulation revealed that the mass did not compromise this vessel, as predicted by the 3D digital assessment and as shown by ICA (Fig. 4).
In recent years, alongside the described multimodal approach, 3D printing technologies have been widely employed in complex cardiovascular scenarios [19]. The 3D models allow the Heart-Team to explore the location, size, and relationship between critical structures and surrounding tissues. Moreover, selecting the 3D printing materials is important and, in our cases, it depends on the surgeon’s requirements. For the two cases, two different 3D printing techniques were used; in the first case, the CAS was printed using color and flexibility to distinguish between the tumor (rigid magenta) from the other cardiac structures (flexible translucent). For the second case, the entire heart (cardiac structures and mass) was printed in the same material and color (light blue). However, for case 2 the model was designed and printed as an assembly to observe possible compression of LMCA and the typical characteristic of cardiac involvement in IgG4-RD. The approach used for both cases was to highlight the mass or tumor, with color, elasticity, or as a separate part. From the surgeon’s perspective, in both cases, differentiating the region of interest (tumor or mass) with color visually aids in evaluation and planning, as other studies have also reported [13, 14].
The 3D models generated from patient-specific data provide our surgical team with insight into real anatomical dispositions and relationships, helping to identify potential complications and develop a unique treatment strategy prior to the operation [20]. However, only a few reports have provided insights into 3D printing and modeling in cardiac tumors. According to search results, in 2008, the first 3D-printed case of a cardiac tumor for surgical planning was reported. After 2015, an incremental trend was seen in the reported studies, presumably due to the use of 3D printing in other surgical practices and easier access to 3D printers [10, 11, 13, 14, 19,20,21,22].
Out of the 8 studies identified in the literature search, three did not report patient follow-up beyond 6 months or local tumor recurrence, while four studies (6/10 patients) provided follow-up data beyond 6 months or 1 year, showing no local recurrence. In only one of the reviewed papers the patient died, which was considered related to the severity of the disease [23]. Most reports utilized 3D models to assess tumor limits, extension, and involvement with cardiac vital structures [19, 21, 22]. Moreover, in some cases, there could be a contraindication to surgery due to an estimated 50% mortality rate based on 2D images [10]. Additionally, the models confirmed the surgical approach and procedure (resection and auto-transplantation), while others indicated a change in the access site [24, 25], or the initial surgical plan [26]. Each study emphasizes a specific variable in the planning process elucidated by using 3D models, such as tumor access site, anatomical position and relationship, unique identification of cardiac structures, or tumor invasion and involvement of surrounding vital structures. It is essential to relate these variables associated with the model, such as the color of structures to highlight tumor extent or to use flexible materials for resection and suturing, as experimented in some reports [22, 27]. As seen in case 2, in scenarios involving tumors and cardiovascular surgery, the focus is not only on generating 3D reconstructed image models but also on guiding the medical team to facilitate optimal decision-making.
Although most studies highlight the positive impact of 3D models on understanding tumor anatomy and surgical planning, the lack of data on model accuracy and direct surgical outcomes limits objective evaluation. Some studies suggest improvements in surgical outcomes, but conclusive evidence of clinical benefits remains sparse. Additionally, the accuracy of 3D-printed models compared to surgical findings relies heavily on the segmentation process. In case 2, we aimed for a more objective approach by measuring the cross-sectional area of the paracardiac mass in the 3D reconstruction and comparing it to the extracted mass (see Fig. 5). Recognizing the limitations of the segmentation process and the paucity of data on the accuracy of 3D models in comparison with surgical findings, as shown in our literature review, there is a clear need for prospective studies with standardized evaluation criteria to accurately assess the efficacy and clinical impact of 3D printed models in cardiac surgery.
Regarding the segmentation software, Interestingly, all studies utilizing 3D-printed models for preoperative planning of tumors or cardiac masses employed specialized software for 3D segmentation and reconstruction, particularly the Mimics Innovation Suite software (Materialise, Inc., Leuven, Belgium). However, more clinical studies are needed to contrast the impact of printed models with control groups, comparing intraoperative variables (e.g., surgery time, medical devices used) and postoperative outcome variables (e.g., mortality, hospitalization, follow-up longer than 1 year), which can also be utilized for cost-effectiveness studies.
The use of 3D printing and/or new technologies for preoperative planning of cardiac tumors is increasing in the literature. However, there is still a tendency to report only case studies, presumably because a prospective study of uncommon cases can be time-consuming. However, more studies with significant samples and their associated clinical and economic impact are anticipated. Finally, we employed the WHO classification for cardiac tumors to standardize the nomenclature of cases, facilitating comparison and exchange of information in for further investigations [27].






留言 (0)