
記住我
This was a single-center, parallel, randomized trial conducted at the simulation center within Children’s of Alabama. Following Institutional Review Board approval, pediatric and internal medicine/pediatric residents were enrolled between November 2020 and January 2023. Trainees between years 1 and 4 were recruited by study personnel via email from the residency program at the University of Alabama at Birmingham/Children’s of Alabama and provided written consent before trial participation. Recruited trainees had to have previously completed The American Academy of Pediatrics Neonatal Resuscitation Program (AAP NRP) training, had at least four weeks of previous neonatal intensive care (NICU) exposure, and had 3 months elapsed since their previous NICU rotation. Participants were compensated with a $10 gift card.
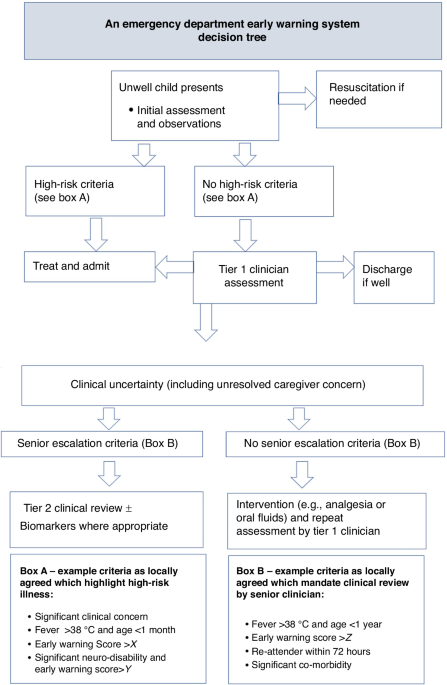
Simulated scenario and randomizationPrior to entering the simulation, participants were provided with the prompt: “You have been asked to attend the cesarean birth of Layla Thomas, a 25-week infant. The mother presented to the Labor & Delivery Unit one hour ago following a motor vehicle accident, no antenatal corticosteroids were given, and the baby will soon be delivered. Prepare for the delivery.”
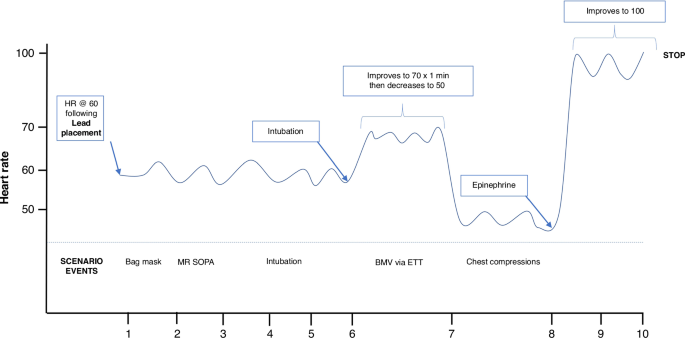
Within the simulated patient room were the manikin (Premature AnneTM, Laerdal Medical, Wappingers Falls, NY), hospital resuscitation cart (containing supplies for airway support, continuous monitoring, and thermoregulation), an Amwell C250 Telemedicine Cart (Boston, MA) adjacent to the bed, and two cameras to provide video recording for subsequent data analysis. So as to evaluate the no-flow fraction, the manikin in the scenario became bradycardic with a heart rate <60 following establishment of effective ventilation with additional time relevant details depicted in Fig. 1. During the first segment of the resuscitation, the heart rate remained between 60 and 100 and the participant received verbal feedback that there was no chest rise prompting the need for corrective bag-mask ventilation maneuvers. One minute after intubation the heart rate decreased to <60 for which chest compressions would be indicated. The heart rate would remain at 50 until endotracheal epinephrine was administered, the heart rate would then increase to >100, and the scenario would conclude. The scenario was stopped after a 10 min duration (given the anticipated ability to perform the simulation’s objectives within this time frame) or upon bradycardic resolution whichever occurred first. Both groups received a debrief at the resuscitation’s conclusion using the “debriefing with good judgement” model.13
Fig. 1: Changes in vital signs during the simulation.
The noted changes in heart rate characteristics over time are indicated in response to participant interventions.
Randomization was implemented using 1:1 ratio with a permuted-block randomization (with blocks of two and four) with the groups: teleneonatal resuscitation and routine resuscitation. Sequentially numbered, sealed opaque envelopes were used to conceal participant group allocation with computer-generated allocation sequences. Envelopes were opened just prior to participants’ entry into the simulation. Stratification was performed by post graduate year (PGY; PGY-1 and PGY-2/3/4). Participants could not be masked to intervention given the study design in which the teleneonatologist interacted with participants in the intervention arm. Study personnel assessing outcomes from video recordings were masked to randomization by elimination of audio recordings and the presence of the telemedicine cart within the visual field irrespective of randomization group.
InterventionAfter signing consent, participants completed a pre-simulation questionnaire indicating the level of training as well as experience with neonatal resuscitation. Those randomized to teleneonatal resuscitation also completed a post-simulation questionnaire with qualitative responses regarding the teleneonatal resuscitation. The same neonatologist was the facilitator for all participants randomized to teleneonatal resuscitation to minimize facilitator variability. The teleneonatologist was instructed to allow the participant to lead the resuscitation but to provide directive communication in instances wherein participants did not timely adhere to guidelines from the AAP NRP1 or failed to provide indicated interventions. The teleneonatologist only had access to information gained from visualization via the Amwell cart. The teleconnection occurred simultaneously with trainees’ entry into the simulated scenario. A research nurse assisted participants in the resuscitation by providing both nursing and respiratory therapy clinical responsibilities in the teleneonatal resuscitation group. Participants randomized to the routine resuscitation group were only supported by a research nurse. An additional research nurse present in both randomization groups became available to provide code epinephrine when requested by the participant.
Study outcomesStudy measures considered in this investigation have demonstrably influenced patient outcomes or are a component to standardized resuscitation guidelines. The primary outcome was no-flow fraction defined as time without chest compressions divided by the time without spontaneous circulation when the heart rate was <60. Improvements in cardiopulmonary resuscitation inclusive of the no-flow fraction have been associated with a return of spontaneous circulation14 and survival.15
Secondary measures included aspects of respiratory support including the use of corrective measures to bag-mask ventilation (e.g., mask adjustment, repositioning the airway), the time at intubation, the frequency of intubation attempts, and the no blow-fraction. The no-blow fraction was calculated as the proportion of time an infant did not receive bag mask ventilation while the heart rate was <100. Additional secondary outcomes regarding cardiac resuscitation included time at which chest compressions were initiated, synchronization compliance, whether epinephrine was administered. All assessments were made using video recordings of participants’ performance masked to teleneonatologist presence.
Participants randomized to teleneonatal resuscitation completed a post-resuscitation questionnaire in which they indicated whether having a teleneonatologist improved the quality of resuscitation in addition to responses related to the audio and video quality and whether any issues with connectivity occurred. Free text comments were also provided.
Power calculationSimulated studies in other populations have reported a control group no-flow fraction of 0.19 (±0.10) in the setting of cardiopulmonary arrest.8 Using an alpha value of 0.05, 80% power, and an enrollment ratio of 1, a sample size of 50 participants would be needed to detect an 8% absolute risk difference (or 32% relative decrease) in the no-flow fraction. An additional 10 participants (5 per group) were recruited to account for the potential inability of video recordings to adequately assess for the primary outcome.
Statistical analysisBinary covariates were compared between groups using the Fisher exact test. For continuous measures, a Kolmogorov-Smirnov test of normality was performed after which the appropriate parametric or nonparametric test was conducted. In instances in which continuous data from only one randomization group were not normally distributed, data were log-transformed and then analyzed. No interim analyses were conducted during the study. The primary outcome was measured per intention-to-treat analysis. No adjusted analyses were performed on any study outcome. Analyses were performed using IBM SPSS Statistics Version 29.0 (Armonk, NY). A two-sided p-value < 0.05 was considered significant. For qualitative analyses research, personnel coded participant responses for specific themes with corresponding quotes.
留言 (0)