Study design
EXPRESS (Expressing in PREmaturity–Simple interventionS) was an unmasked, parallel group, multi-centre, randomised, controlled trial conducted in four United Kingdom hospital neonatal units. The study was funded by the National Institute for Health and Care Research (NIHR). It was approved by the Bloomsbury Research Ethics Committee, London (21/LO/0279) and registered as ISRCTN 16356650. The trial protocol has been published.19
Participants
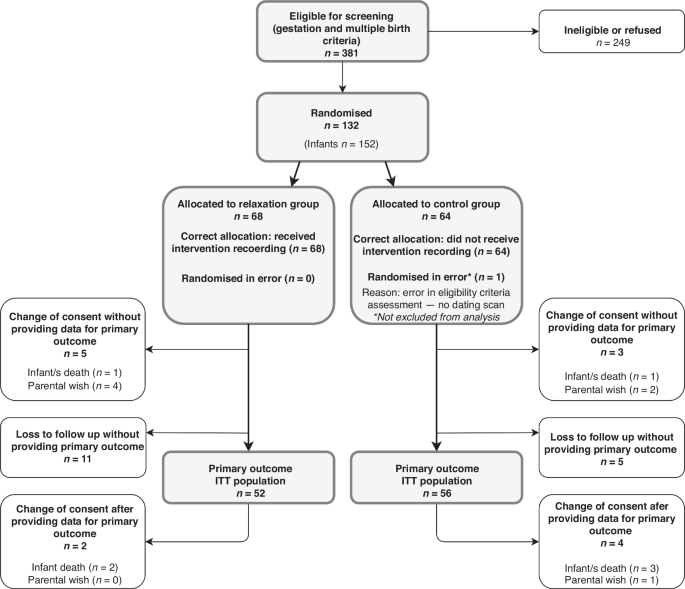
Inclusion criteria were birth between 23+0 and 31+6 weeks’ gestation within the previous 3 days; being 18 years or over; intention to express milk for at least 2 weeks; able to give informed consent; and having a device on which to listen to an audio recording. Exclusion criteria were lack of antenatal dating scan and more than two infants. Participants gave written, informed consent on paper or electronically. There were no language constraints specified. Interpretation services were not available, but potential recruits could use their support networks for assistance if needed.
Three English National Health Service trusts were involved, including three tertiary and one local neonatal unit. All sites have hospital-grade breast pumps, a free home loan scheme, dedicated infant feeding and psychological support staff, and provision of donor human milk with varying criteria for use. Two trusts have neonatal UNICEF Baby Friendly Initiative (BFI) UK level three accreditation, suggesting a good level of lactation support. Clinical support was not standardised between sites, as this was considered to represent real-world standard care.
Randomisation and masking
Participants were randomised (with 1:1 ratio) by site staff using a web-based randomisation system incorporating allocation concealment. The allocation sequence was computer generated by a statistician using randomly permuted stratified blocks of size two and four (using Stata v15.1). Stratification was by recruiting site, gestational age at birth (23+0 to 27+6 or 28+0 to 31+6 weeks) and number of infants (one or two).
Procedures
The control group received clinical lactation support from neonatal staff. The intervention group received clinical support and a 12-min audio file (Supplementary Audio File 1). They were asked to listen to the recording several times a day while expressing milk. The recording was modified from a soundtrack used for previous studies20 in order to ensure that it was appropriate for mothers of sick infants who had never breastfed (rather than the original audience of mothers of healthy breastfeeding infants); the modification process is described elsewhere and involved parent collaborators.21 The recording includes breathing exercises, muscle relaxation, and visualisation of milk flow and infant skin-to-skin contact.
Baseline questionnaires were submitted by participants and site staff. On days 4, 14 and 21 after birth, participants recorded each time they expressed milk for 24 h and answered questionnaires, including frequency of listening to the recording.
Participants weighed milk using a portable scale with 0.1 g accuracy (Kabalo). Accuracy with the scale was confirmed by researcher contact between days 4 and 7. Participants responded to SMS (short messaging service) messages at 36 weeks’ postmenstrual age (PMA) and 4 months’ corrected age (CA) to report feeding status. At 36 weeks’ PMA this data was extracted from medical notes if there was no response. Demographics of the potentially eligible population were extracted from routinely entered clinical data.
To maximise efficiency in the available time, participants in the final 22 weeks of recruitment completed the trial at 36 weeks’ PMA. This affects one of the secondary outcomes (exclusive MOM at 4 months’ CA).
The trial contributed to a doctoral thesis and was supported by a Clinical Trials Unit and an independent Trial Steering Committee. An extensive process of Patient, Public Involvement (PPI) is described elsewhere.21
Outcomes
The primary outcome was the highest 24-h expressed MOM weight recorded on any of days 4, 14 or 21. These timepoints were chosen because of prior work showing a close association between early milk yield and longer-term lactation outcomes in the NICU setting.22,23 Secondary outcomes were expression of at least 750 g of MOM on any of days 4, 14 or 21; expression rate (milk quantity per minute of expression) at day 21; mental health measures at day 21; any and exclusive MOM at 36 weeks’ PMA and exclusive MOM at 4 months’ CA. Mental health measures were the Spielberger State-Trait Anxiety Index (six item format; STAI-6) and the Post-traumatic stress Checklist for DSM-5 (PCL-5). The STAI-6 was administered at baseline and day 21. The PCL-5 was administered on day 21 only as this checklist applies to experiences in the weeks following a traumatic experience and therefore cannot be administered at baseline. Process indicators were skin-to-skin contact duration, expressing frequency and duration.
Statistical analysis
The trial was powered to detect an increase in primary outcome from 670 to 825 g (SD 300 g), with 80% power and a two-sided significance level of 0.05. This is a smaller effect size than seen in the meta-analysis.15 The control group estimate was informed by local audit data. With 10% attrition expected, the recruitment target was set at 132.
There was a pre-specified statistical analysis plan. For continuous outcomes, this was linear or quantile regression as appropriate, and for binary outcomes log binomial regression or Poisson regression with robust variance estimator if the model failed to converge. Analyses were adjusted for the stratification factors where possible. The STAI score at day 21 was adjusted for baseline score. The primary outcome was adjusted for the associated measurement day (the day that the highest milk weight was recorded).
Participants were analysed in the groups to which they were randomly assigned (the intention to treat the population). Primary analysis was on a complete case basis. Exploratory subgroup analysis used the statistical test of interaction to examine the heterogeneity of treatment effect on the primary outcome by gestational age at birth. Other analyses were summarised by allocation with no comparative statistics, to limit multiple comparisons; statistical inferences were limited to eleven. Exploration of the association of adherence and relaxation perception with the primary outcome was pre-specified, without comparative statistics.
Sensitivity analyses were planned to explore the pattern of missing data for the primary outcome using multiple imputation and pattern mixture models; and by re-defining the parameters of the primary outcome. The four sensitivity analysis redefinitions of the primary outcome were 24-h milk weight on day 21, highest 24-h milk weight on day 14 or 21, excluding records with fewer than four expressing sessions, and excluding records submitted more than 48 h late. The pattern mixture model imputed missing primary outcomes as the average value plus a delta value of −200 g to +200 g, modelling potential bias of missing data by up to 200 g.
Post-hoc random effects meta-regression of milk quantity and gestational age at birth combined the results of this study with neonatal unit studies16,20,24,25,26,27 included in a recent meta-analysis,15 using variance-weighted least squares technique. All study effect estimates for milk quantity were expressed as standardised mean differences. Between-study variance was estimated with residual maximal likelihood. Stata v18 was used for analysis.
The Data Monitoring Committee reviewed one interim report. There were no formal stopping guidelines due to the trial size.

留言 (0)