We hypothesised that a comprehensive and multi-source overview of drugs with AKI potential, which integrates expert consensus, SRS databases, DIDs, and NephroTox, would lead to the generation and characterisation of a robust list of drugs with AKI potential. Our approach involved a wide-ranging effort in the field of DAKI, tapping into knowledge sources like SRS databases, DIDs or NephroTox that had remained underutilised in previous investigations. Through our analysis of four expert consensus studies on drugs with AKI potential, we found moderate to very strong agreement for 63 drugs. Disproportionality analyses conducted on three SRS databases largely showed consistency for these 63 drugs, likely because healthcare professionals tend to report what they know. As expected, higher variability in ROR signals was observed for drugs with moderate agreement. Average AKI ADE frequencies from the analysed DIDs exhibit lower levels of consistency with medical experts compared to ROR signals, albeit different reporting patterns can be identified in moderate compared to strong or very strong expert agreement levels. This underscores the effectiveness of our novel approach, extending beyond conventional methodologies, and focussing on previously underexplored dimensions of drugs with AKI potential.
4.1 Expert Consensus Lists of Drugs with AKI Potential
The 63 drugs with AKI potential that have surfaced from the four expert consensus studies, represent a broad spectrum of therapeutic agents, with antibacterials, antivirals and NSAIDs emerging as the most frequent pharmacological drug classes. Indeed, there is ample evidence that drugs belonging to these classes may cause AKI [22, 23, 43], which has also been reflected in clinical practice guidelines [1]. On the other hand, we identified 131 drugs with limited agreement between the lists presented in the four expert consensus studies. This limited agreement may arise from various factors, including differences in the primary sources used, the composition and background of the expert panels, methods for achieving consensus, and the lack of a standardised definition for what constitutes a drug with AKI potential.
While consensus-reaching processes involving expert knowledge should always be grounded in a robust scientific evidence base [44], this may not always be the case in the field of DAKI. In fact, the current evidence base for AKI potential of many drugs is often found to be weak and biased [19]. Even for drugs such as vancomycin, which have long been considered as nephrotoxic, it has been noted that stronger evidence is still required judging from currently available evidence [45, 46]. Against this backdrop, novel methods, like the target-trial emulation framework, hold the promise to improve the design of observational studies to better ascertain the AKI potential of drugs [47]. This can help to address, amongst other biases, those caused by insufficient adjustment for confounding factors, such as concurrent use of other medications, drug-drug interactions, and underlying acute states like multi-organ failure.
The above may also explain why drugs such as glibenclamide, metoclopramide or metformin, which do not seem to exhibit AKI potential based on the current evidence [34, 35], appear inconsistently across expert consensus lists. Here, we suspect that the expert consensus studies may have conflated AKI risk and non-AKI side effects resulting from drug accumulation due to inadequate dosing adjustments for kidney function. In fact, if the dose of these drugs is not adjusted for reduced kidney function, they can result in various other non-AKI side effects [48]. Second, some drugs like integrase strand transfer inhibitors (e.g., dolutegravir [49]) or tyrosine kinase inhibitors [50] (e.g., imatinib or sorafenib) can elicit an increase in serum creatinine without causing kidney damage or dysfunction (i.e., also referred to as pseudo-AKI) [8]. Current evidence suggests that drugs like these may be blocking the uptake of serum creatinine from the blood without altering the glomerular filtration rate by inhibiting the drug efflux transporters, such as organic cation transporter 2 (OCT2) and multidrug or toxin extrusion (MATE) transporters 1 organic cation transporters [49, 50].
4.2 Disproportionality Analyses using SRS Databases
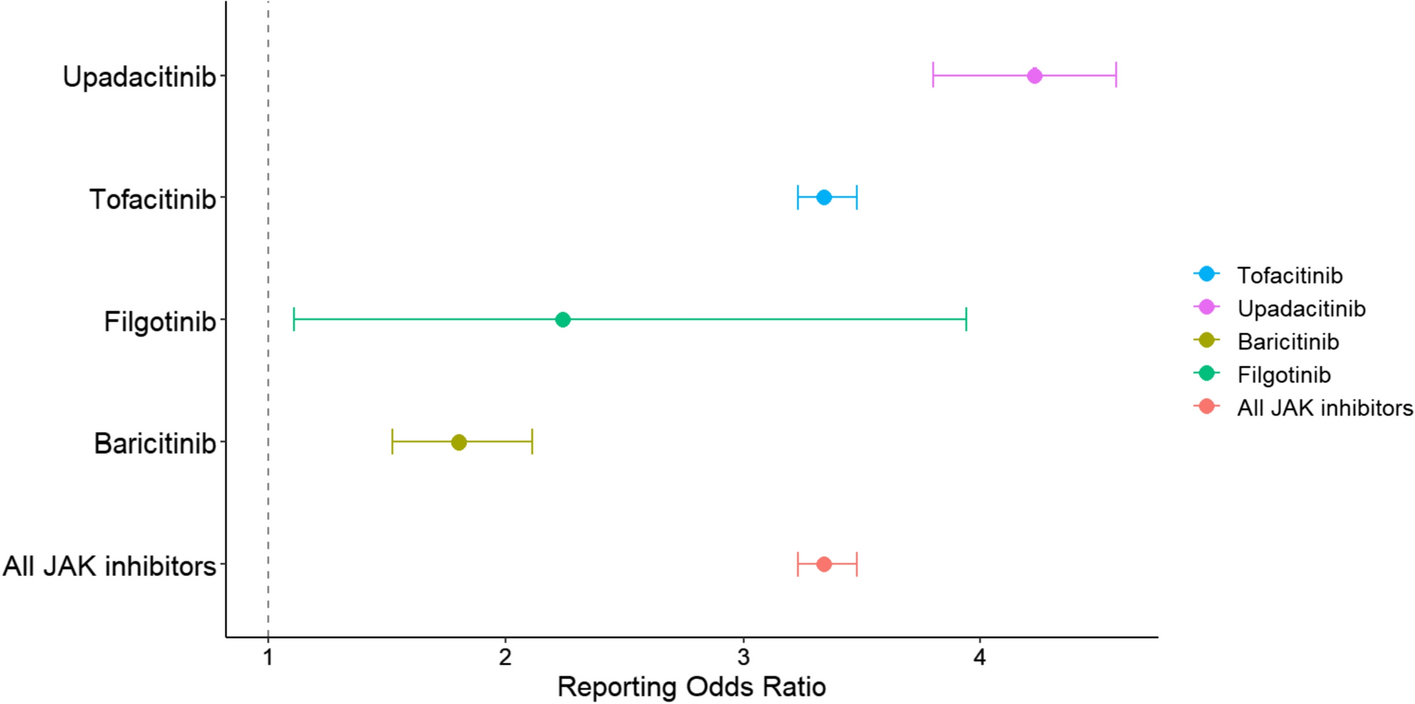
We note that strong associations with AKI found for antiviral drugs like aciclovir [24, 26, 51, 52], antibacterials like gentamicin [25, 51], vancomycin [24,25,26] and colistin [25] or NSAIDs such as diclofenac [24, 26, 51, 52] and ibuprofen [26, 51, 52] are aligned with other pharmacovigilance studies using the FDA Event Reporting system (FAERS) database [25, 26], the Japanese Adverse Drug Event Report (JADER) database [24] and the French National Pharmacovigilance Database (FPVD) [51]. Interestingly, in our analysis, RAAS inhibitors exhibit significant ROR signals in practically all cases, which indicate strong associations with AKI. However, RAAS inhibitors should be considered nephroprotective, as a decrease in eGFR caused by RAAS inhibitors is considered an acceptable haemodynamic change and a sign that these drugs are ‘doing their job’ rather than a sign of AKI in the absence of severe bilateral renal artery stenosis, volume depletion or administration with a possible pharmacodynamic drug-drug interaction (i.e., triple whammy) [8]. This is similar for diuretics, which are not considered to cause AKI, and only become a concern when used excessively, leading to sustained volume depletion or contribute to a pharmacodynamic interaction. In fact, prudent use of diuretics to prevent volume overload has been associated with improvements in the kidney function [39].
Furthermore, we identified drug classes with high variability in ROR signals like PPIs. Indeed, PPIs are currently subject of discussions [21, 53], as their safety profile was recently challenged by epidemiological and histological studies [21, 53, 54]. In its turn, and as a limitation of disproportionality analyses, this could have led to ADE-stimulated reporting or masking effect and potentially end up biasing the signals. Thus, as a general remark, disproportionality studies should only be used for hypothesis generation and further causality studies are warranted to ascertain a relationship with AKI [39].
It should also be noted that in the disproportionality analyses we have discarded ICSRs associated with AKI containing more than one INN, which may be clinically relevant, thus leaving this exploration for future work. In addition, some signals in CVAR were not reportable due to low number of ICSRs, but these can be complemented with the signals present in the other SRS databases analysed.
4.3 Average AKI-related ADE Frequencies from DIDs
The higher variability in AKI-related ADE frequencies observed in DIDs compared to disproportionality analyses signals may be influenced by differences in content refresh rates. Drug information databases tend to be updated at longer time intervals in contrast to disproportionality signals, which can be tracked virtually continuously. This emphasises the need to consider the temporal aspect and diverse data sources when assessing the AKI potential of a drug [55, 56]. Consulting multiple information sources which adds value to our resource. The case of NSAIDs is of particular interest, as strong associations with AKI observed in most disproportionality analyses are not mirrored in DIDs. We speculate that this may be reflective of the low prevalence of NSAID-induced serious AKI events (estimated to be between 1 to 5%) [57], possibly due to the prescribers’ awareness of their AKI potential for patients at risk for AKI. As for the variability in AKI-related ADE frequencies observed between DIDs, the differences in the type of evidence considered and the critical appraisal of evidence may provide an explanation. Drug information databases do not account for specific populations and therefore they could provide wide ADE ranges. We have carried out manual mappings for the DIDs, which did not support MedDRA® terminology. Whilst we have provided a detailed account of this process, it is indeed an ongoing area for improvement.
4.4 NephroTox
By employing NephroTox, we found that most drugs with AKI potential are consistently present in published studies where adverse kidney events are reported. Following the method of Welch et al [26] to identify drugs with AKI potential, the drugs under investigation in this study are ‘known’ for their association with AKI potential.
4.5 Integration of Knowledge from the Four Sources
We envisage our resource as a tool to be used for aiding AKI potential assessment when developing expert consensus lists of drugs with AKI potential and also as decision support when prescribing drugs in routine care. In this respect, we have encountered a number of cases where our resource may have changed the opinion of the experts, had our resource been available to them at that time. For example, our resource shows that amoxicillin and beta-lactamase inhibitor (i.e., clavulanic acid) displays moderate agreement, but no AKI signal is detected using any of the three SRS databases and ADE frequencies in the DIDs included tend to be very low. Given this pattern, the inclusion of amoxicillin and beta-lactamase inhibitor on the list of drugs with AKI potential is up for discussion. Potentially, this could also be said for drugs like ioversol or sulfasalazine.
Finally, we acknowledge that the AKI potential of drugs may be confounded by multiple factors (e.g., polypharmacy patterns) that may obscure the underlying biological process. Therefore, formal causality assessments are needed to assess whether AKI was indeed caused by a drug [12]. Thus, our resource serves as a starting point to signal potential associations between drugs and AKI and prompts further studies on specific areas, rather than being a conclusive endpoint.
From a practical standpoint, successful attempts have been made to automate knowledge-based generation for identifying ADEs [58]. However, the automation of knowledge retrieval from the knowledge sources leveraged in this study may be challenging at different stages in the analysis pipeline due to difficulties in data extraction or parsing processes. For instance, access to EV ICSRs data is layered and drug name standardisation is required for DAEN or CVAR databases. In addition, some DIDs do not support MedDRA® terminology (i.e., FK, IM, Micromedex®) or display high data missingness (i.e., SIDER). The latter DID does not entail curation by medical experts as is the case for the other DIDs. Therefore, continued improvements in data collection policies and terminology standardisation are needed to ensure compliance with findability, accessibility, interoperability and reusability (FAIR) principles, which enable progress in research. Whilst automating the integration of sources remains unfeasible at present, it is imperative to closely monitor the accrual of evidence for drugs whose AKI potential remains uncertain.
4.6 Strengths and Limitations
This study has several strengths. First, the integration of diverse and disjointed, often underexplored, knowledge sources has facilitated a comprehensive investigation on drugs with AKI potential from different angles. Second, by combining pharmacovigilance data from different regulatory agencies and DIDs across multiple countries, our resource provides a thorough overview of 63 drugs with AKI potential. Third, besides Dutch information sources, we have also included Micromedex® as a globally recognised DID and assessed diverse SRS databases like EV, CVAR and DAEN. This, coupled with broad alignment with previous studies, strengthens the generalisability of our findings and helps to reveal areas that require further investigation. Our resource and its scope are relevant to capitalise on the strengths each knowledge source has to offer and mitigate their limitations, as highlighted in the literature [59].
Our study also has several limitations. Starting with our literature search, we only searched the Medline database and focussed on drugs approved in the Netherlands. However, we identified a sufficient number of high-quality, peer-reviewed studies, which allowed us to allocate more time to other information sources included in this study. The 63 drugs included in this study are also common in other countries [16,17,18,19]. Second, we have used as input existing expert consensus lists of drugs with AKI potential, which may have led to the omission of some drugs with known AKI potential. One such example worth mentioning here may be antitumour drugs like azacytidine, streptozocin, high-dose pemetrexed and pentostatin, which exhibit AKI potential based on current evidence [34,35,36]. Presumably, these drugs may have been overlooked in the process of gathering expert consensus in the included studies. Furthermore, by taking existing expert consensus lists of drugs with AKI potential as a starting point, our resource may be less likely to include new therapeutic agents with AKI potential. In addition, both disproportionality analyses and DIDs necessitate extended periods of time to accumulate sufficient data in order to prevent temporal biases [39, 60] and ultimately provide robust estimates. This illustrates the importance of conducting this type of exercise periodically, whilst recognising that domain knowledge retrieval automation may not always be suitable for new therapeutic agents. Fourth, in relation to disproportionality analyses, we have included all ICSRs, as information on formal causality assessment [61] was not available in the SRS databases used. It is important to note that disproportionality analyses only provide an indication about the reporting rate of an ADE and do not necessarily carry a causal consideration, so the signals found are merely associational and cannot be used as evidence for a causal relationship. Fifth, all knowledge sources have been pulled together into a single resource giving the appearance of being on an equal footing. Indeed, the number of studies identified via NephroTox may not be as relevant for assessing AKI potential as ADEs frequencies from DIDs or disproportionality analyses, because it is an aggregated statistic that does not consider the quality of evidence in the studies found. To remediate this, we have provided contextualisation and emphasised the most salient features of the resource components.
4.7 Future Research
We consider our resource as a stepping stone to consolidating a list of drugs with AKI potential. Thus, the characterisation of the 131 agents labelled as having limited agreement in our study using SRS databases, DIDs and NephroTox (as we did for the 63 drugs labelled as having at least moderate agreement), is left for future research. Indeed, sufficient data accrual and mechanistic considerations based on existing evidence should also play a role in the prioritisation for analysis of each of these drugs. With regard to antitumour drugs with AKI potential that we have not assessed in this study (e.g., azacytidine, high-dose pemetrexed, pentostatin, streptozocin), a potentially interesting approach to tackle this issue could be following the reverse process, that is, starting by mining information about AKI potential of drugs in the empirical data sources (like those we propose in our study) and involving experts to discuss the existing evidence at the end.

留言 (0)