
記住我






Foreign body aspiration and ingestion are rare complications of oral medicine. Various oral treatments can lead to aspiration and ingestion, including root canal treatment, implant surgery, tooth extraction, denture restoration, orthodontic treatment, etc. Foreign bodies include root canal treatment instruments, implant parts, implant screwdrivers, dental drills, crown and bridge restorations, orthodontic devices, rubber dams, and even dental mirrors and needles [11,12,13,14,15,16]. They usually occur in children [17] and the elderly [8, 11].
Reports of accidental inhalation or swallowing of orthodontic appliances are rarely seen, mainly because most orthodontic appliances are bonded to teeth. Even if they fall off, brackets with small size and smooth surface can mostly be discharged smoothly from the digestive tract with food. Also, orthodontic removable appliances, large in size and elastically retained by clasps or other structures, are usually hard to swallow. The most common cases were caused by expansion keys [2, 3] and archwire segments [4,5,6]. Some other orthodontic appliances often swallowed are children’s space retainers, brackets [7], buccal tubes [6] and bands [8] when they are not firmly clamped during bonding or loosened during usage. Devices vulnerable to fracture are also easily ingested such as welding parts of metal appliances [9], or weak structures of the plastic appliances [10]. In addition, accidental aspiration may also occur when making orthodontic alginate impressions. If inhaled when the impression material has not yet solidified, it may enter deeper structures like bronchi and alveoli, leading to pulmonary dysfunction and necessity for lobectomy [18].
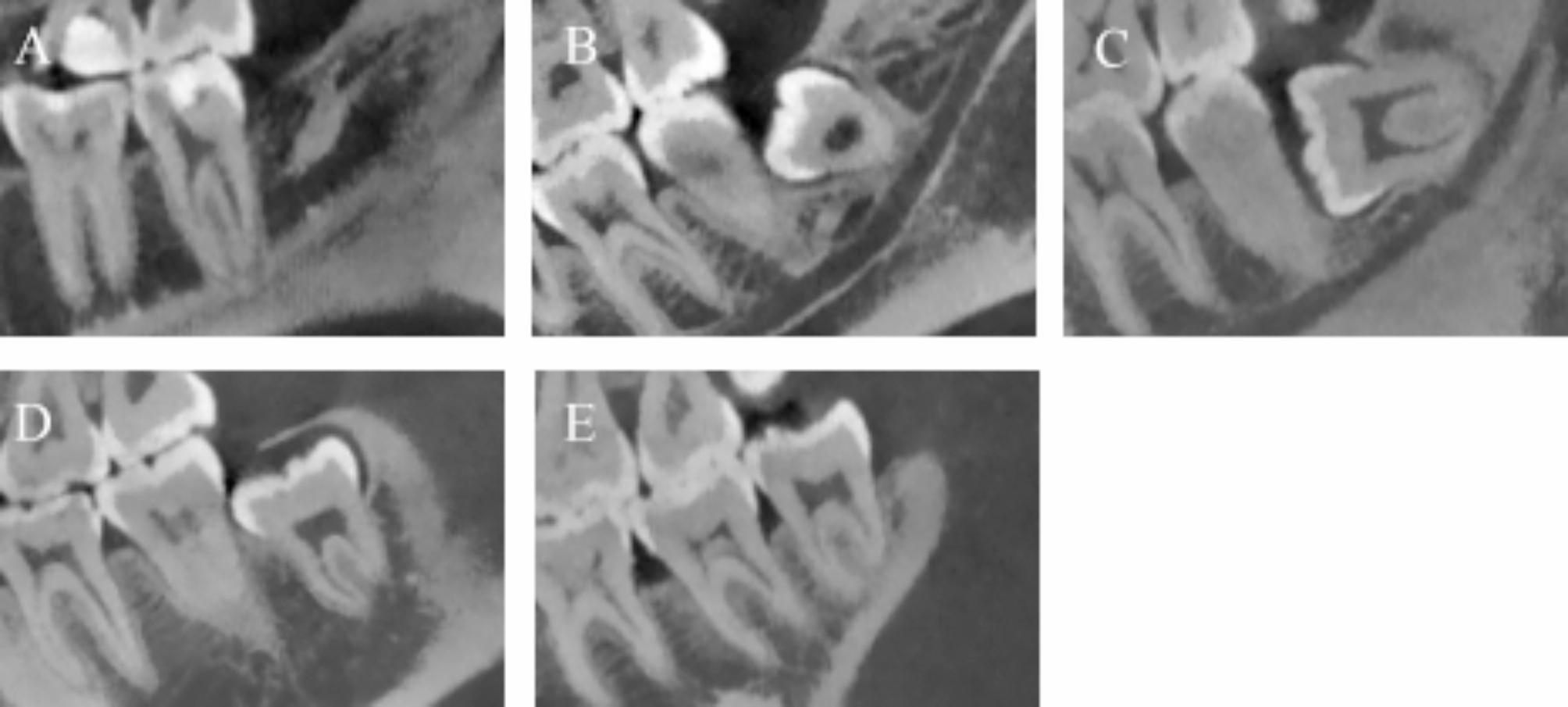
For aligners, apart from the inherent properties of the material itself, external forces and wear are the main causes of aligner fracture [19, 20]. In this case, at the beginning, the occlusal contact were concentrated in bilateral molar areas (Fig. 1D, E), increasing the possibility of abrasion of the aligner in molar segment. In addition, the buccal and lingual border of the fractured aligner piece was cut out for the space of buttons bonded on buccal and lingual surfaces of molars for intrusion purpose (Fig. 5B), leading to a decrease in retention force and ended up falling off when drinking. On top of that, prolonged wear of a single set of aligner, excessive force applied by the patient when putting on and removing the aligner, wearing the aligner while eating and use of hot water or chemical cleansers may also reduce the life span of aligners [19, 20].
OutcomesReports show that about 87% of instruments are swallowed into the digestive tract, and 13% are inhaled into the respiratory tract [21]. Inhalation into the respiratory tract is usually more dangerous and more difficult to treat [21], and there is almost no possibility of natural expulsion [2]. Common aspiration symptoms mainly include inability to talk, cough, wheeze, dyspnea and loss of consciousness and other severe respiratory obstruction manifestations [22]. Some small objects entering the respiratory tract may be asymptomatic for a long time, but may have serious consequences in the long run [23]. The success rate of bronchoscopic removal of foreign bodies in the respiratory tract is 99%, but there are still 2.4–5% rate of complications [24]. 90% of swallowed foreign bodies can pass through the digestive tract successfully, but about 10% of cases require endoscopic removal of foreign bodies, and 1% require surgical removal [25,26,27,28]. If it enters the digestive tract, the sharp edges of the metal and plastic fractures can scratch the esophagus and adjacent tissues, which both are dangerous and should be treated in time.
Diagnosis and treatmentWhen a foreign body enters the mouth by mistake, the doctor should immediately keep the patient calm and remove the foreign body as soon as possible. Orthodontists and general dentists must be vigilant in recognizing signs and symptoms of airway obstruction such as inability to talk, cough, wheeze, dyspnea and loss of consciousness in case that any dental object is lost into oropharynx [10]. If it is no longer visible in the mouth, imaging examinations should be conducted to carefully evaluate the location of the foreign body to determine whether it has entered the digestive tract or respiratory tract and the subsequent treatment plan [12, 29].
If dental instruments and devices enter the airway with no dyspnea, it is not recommended to inducing coughing, performing Heimlich maneuver, patting the back or using any external forces [10]. Instead, the patients should be kept still and delivered to a general hospital immediately. If breathing difficulty occurs, an ambulance should be called immediately, and cricothyroidotomy or tracheotomy should be performed in severe cases. If it enters the esophagus, excessive swallowing should be avoided to mitigate pain and further lesions to esophagus.
To determine the treatment plan, imaging is very necessary to confirm the location, size and adjacent relationship of the foreign body [30, 31]. If the foreign body enters the respiratory tract or is obstructed in the esophagus, it needs to be removed in time, because it is almost impossible to expel it by itself [2] and the esophagus is adjacent to important anatomical structures such as the aorta. The special feature of this case is that commonly swallowed dental instruments often contain high-density components such as metal and ceramic, while orthodontic invisible aligners are made of transparent plastic, which has low density and low X-ray opacity. Therefore, the emergency department lacks experience in reading radiological images of this case and at first, no foreign body was found in the commonly used soft tissue window. The location of the foreign body was determined only after adjusting the gray value range to lung window, which promoted the positive determination of the treatment plan. Therefore, for invisible braces, impression materials, resins and other materials with low X-ray opacity, CT should be taken and the lung window should be selected for image reading.
If a foreign body enters the digestive tract, generally speaking, most can be discharged asymptomatically. But for a sharp device, the longer it stays in the body, the more likely it is to cause local tissue perforation and thus cause serious complications. Therefore, early location of the position and in-time removal of the foreign body are suggested [5, 9, 32]. It has been reported that to remove a foreign body by endoscopy, the best time window is within 2 h and no later than 6 h [33]. If delayed, the foreign body may pass through the pyloric sphincter and enter the duodenum [33]. If it enters the stomach, it is usually necessary to observe the patient for clinical discomfort and other symptoms for at least 1 week, and perform a series of imaging and fecal examinations. If the foreign body enters the intestine, it needs to be closely observed until the foreign body is expelled [34]. During the observation period, the patient can have high-fiber foods and closely inspect the clinical symptoms to avoid intestinal perforation, in which case, surgical intervention is required. In a word, the patient needs to be actively followed up.
PreventionTo reduce the incidence of foreign body ingestion and aspiration during treatment, prevention should be the priority. What follows are clinical recommendations for doctors.
• After installing the dental drills, doctors should turn it on for 20 to 30 s away from the patient to test if it is working properly. If the drill swings, rotates abnormally, or falls off, it needs to be adjusted or changed in time.
• Orthodontists should use needle holders to clamp the archwires, and use reversed forceps (Fig. 6) to clamp the brackets and buccal tubes rather than traditional forceps to prevent them from falling off [35].
Fig. 6
Traditional dental forceps and orthodontic reversed forceps. (A) Traditional dental forceps; (B) Orthodontic reversed forceps; (C) A reversed forcep holding a buccal tube
• For handheld micro-instruments that patients need to use at home, such as the expansion key, patients should be instructed to use silk threads or dental floss to tether the instrument tightly from outside the mouth if permitted.
• The removable devices should be designed to an adequate size, making it harder to be swallowed.
• When designing the aligners, the attachments and buffer areas should not be too large, as this may affect retention and strength.
• Doctors should teach patients the appropriate way to put on and take off the removable devices to reduce material fatigue caused by external forces.
• Removable devices should be ensured to have sufficient retention before placing in patient’s mouth and supervised on every regular visit.
• The invisible aligners and retainers, due to their fragile structure, are easily damaged and fractured after wearing for a long time, so patients should be informed to return for follow-up visits in a timely manner and doctors should replace the appliances with compromised retention and strength as soon as possible.
There are also some advises for patients.
• Patients should avoid using hot water or chemical cleaners to clean the removable appliances, as this can cause the deformation and weaker strength.
• Patients need to maintain regular and timely follow-up visits.
• To avoid accidental ingestion, patients need to be told that when poor retention, crack or fracture occurs in any appliance, they should contact the attending doctor immediately and do not continue to wear it.
• Once ingestion or aspiration happens, they should go to the emergency department for examination and treatment in time to reduce the occurrence of complications.
留言 (0)