This study aimed to assess the diagnostic potential of the FM for identifying the causal jaw in Class II Division 1 malocclusion comparing it with lateral cephalometry, which is considered the reference standard. Notably, Paduano et al. [12] demonstrated that a patient performed FM in the context of Class II Division 2. However, our study exclusively included patients with Class II Division 1 malocclusion. This selective inclusion was deliberate, as division 2 presents challenges due to palatal incisor inclination, obstructing mandibular displacement and serving as a physical barrier to the FM [13]. The causative jaw was determined using the Steiner and McNamara analyses. Notably, the majority of our sample (60%) exhibited mandibular retrusion, while 40% displayed maxillary protrusion. These proportions closely align with the typical distribution observed in the general population for subjects with normal Angle Class II malocclusion [2, 14, 15].
According to the results, approximately half of the orthodontists in the study relied solely on cephalometry to identify the causative jaw in Angle Class II. Approximately one-third use a combination of cephalometry and clinical methods, such as FM or an extraoral facial examination. The remaining small minority depends on clinical methods alone. Notably, while there is limited information in the scientific literature regarding the distribution of diagnostic methods used, soft tissue and aesthetic assessments are considered crucial in modern orthodontics for evaluating cephalometric parameters [16]. Because of the individual variances in thickness of the soft tissue, it is shown that it has a significant influence on facial profile and behaves independently from the underlying skeleton [17]. This could explain the different results between the cephalometrics and FM evaluation. Finding out which analysis is best suited to achieve diagnosis and, in turn, a suitable treatment plan, becomes relevant. The needs of orthodontic patients are mostly aesthetic needs [17], and one of the potential advantages of FM is the possibility of evaluating the perceived facial aesthetic. On the contrary, skeletal pattern imbalance does not necessarily correspond to undesirable aesthetics.
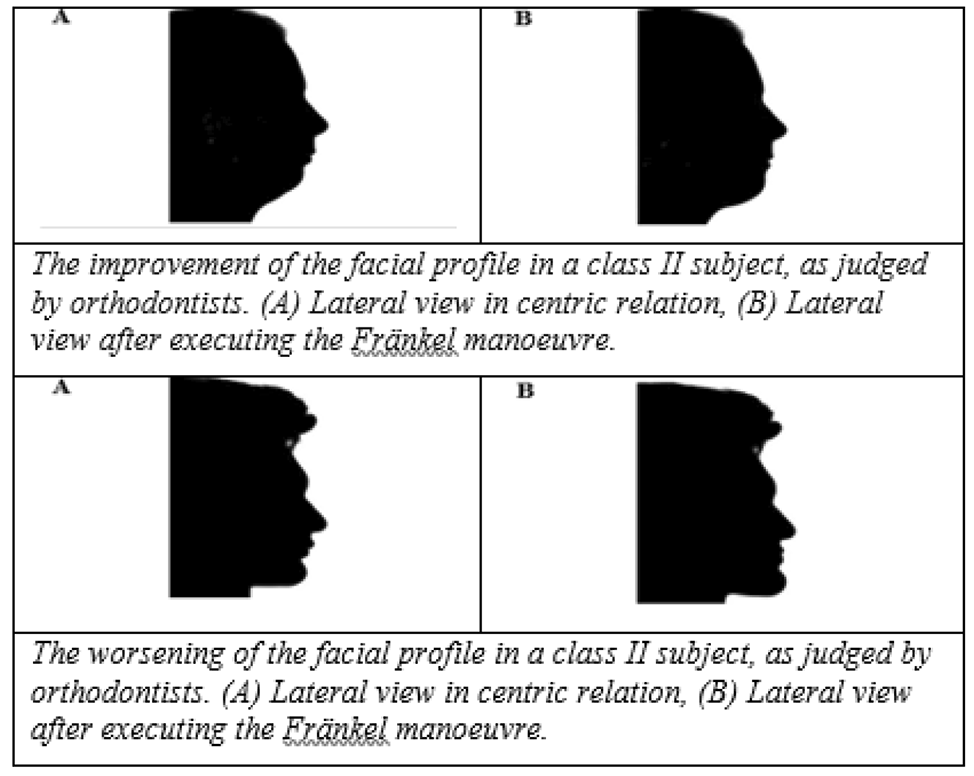
The influence of FM on facial aesthetics was investigated among Lithuanian GP dentists and orthodontists. According to the results of this study, the mean improvement score after the manoeuvre was significantly greater for mandibular retrusion than for maxillary protrusion, as assessed by both orthodontists (29.4 vs. 5) and GPs (21.4 vs. 13.5). These findings are consistent with those reported by Ahrari et al. [9]. Therefore, FM is associated with a more harmonious facial profile and significantly better aesthetics in patients with a retrognathic mandible and a normal maxillary position. Deterioration of the profile during FM is associated with a biprognathic jaw position, where the mandible adapts to the protruding (prognathic) maxilla. According to Martina et al. [2], although the assessment of the manoeuvre may seem very subjective, it can be replicated with a high degree of precision, without the need for clinical experience.
In terms of the diagnostic accuracy of the manoeuvre, a higher diagnostic accuracy was observed for the orthodontist group. The prognostic power of the parameters was assessed by the area under the curve (AUC), an index of how well the parameter can distinguish between two diagnostic groups (maxillary prognathia/mandibular retrognathia) [18]. GP dentists rated the sensitivity and specificity of the Fränkel manoeuvre for identifying these diagnostic groups at 72% and 47%, respectively, while orthodontists rated it at 64% and 82%, respectively. The area under the curve (AUC) was 0.62 for GPs and 0.78 for orthodontists. The assessment of the AUC showed that the manoeuvre is not perfect but rather useful for diagnosing skeletal Angle Class II occlusions (mandibular retrognathia or maxillary prognathia). It is crucial to note that achieving 100% accuracy necessitates the entire AUC, and the ROC curve should be fully shifted to the upper-left corner of the graph [19].
The greater diagnostic accuracy of the FM used by orthodontists could be attributed to the experience of the study participants. Among orthodontists, less than one-third had less than 5 years of experience, while almost half (45%) of the GPs had less than 5 years of experience. Ahrari et al. [9] emphasised the importance of matching factors such as the number of doctors, age, sex, and clinical experience to minimise potential confounding effects. Martina et al. [2] categorised doctors into two groups—those with less than 5 years of experience and those with more than 5 years of experience—and found that the difference in scores was not statistically significant (p > 0.05). However, in our study, the groups were not separated by seniority, and the results were calculated under the assumption that clinical experience should not significantly influence the outcomes [2].
In this study, the FM was compared with two-dimensional (2D) cephalometric analysis as a reference standard. Quan et al. [20] performed a meta-analysis investigating the differences and accuracy between 2D and 3D cephalometric tests. They concluded that the accuracy of the images obtained from cone beam computed tomography (CBCT) scans is comparable to that of conventional cephalometric measurements. However, differences between two skeletal parameters (Ar(Co)-Gn, Me-Go) and one dental parameter (U1-L1) were found to be statistically significant between CBCT and conventional cephalograms (P = 0.000, P = 0.004, P = 0.000, respectively). According to Sam et al. [21], to assess the performance of 3D cephalometric landmarks in assessing the reliability of 3D craniofacial complexes, further research is needed. Therefore, CBCT is recommended as a complementary tool when improved diagnosis is needed in the present circumstances and during treatment planning [20].
Rongo et al. [10] conducted a study comparing FM performed on two-dimensional and three-dimensional images. A comparison of the 2D and 3D images revealed that the reliability of the 2D images was greater than that of the 3D images of the FM in stereo photography. This study has several inherent limitations. First, only 10 patients’ photos were included in the study, and the sample size comprising GPs and orthodontists was relatively small; therefore, the work was only eligible for the pilot requirements. Second, there was no accurate validation tool available for identifying the causative jaw in Class II malocclusion patients, as cephalometry also has some limitations in the diagnostic process [4,5,6, 21, 22]. Third, according to Lo Giudice et al. [17], patients who are hyperdivergent, have statistically thicker cortical bone than normodivergent and hypodivergent patients, therefore aesthethic assessment of the FM might differ according to the facial pattern. Finally, the present study design does not allow us to conclude that similar results can be obtained between the outcome of the manoeuvre and the outcome of the treatment.







留言 (0)