In this in vitro study, the HepG2 cell viability was measured after ECT with increasing concentrations of the chemotherapeutic drugs bleomycin or cisplatin, or after CaEP, to determine its efficacy on HepG2 cells in vitro using the ESOPE protocol, compared to non-electroporated drug treatment.
The colorimetric MTT assay, which assesses cell metabolic activity, was used as a representation of HepG2 cell viability [19]. One might argue that relatively high concentrations of bleomycin are used in this in vitro study. However, the concentration range for the drug bleomycin, as well as cisplatin and calcium was chosen to include the dosage used in literature for relevant and comparable in vitro studies, with proven effectiveness [12, 19, 21, 24,25,26]. These studies selected 10 µM bleomycin as optimal in vitro concentration from a test range of 0.1–50 µM bleomycin [21, 24]. In addition, the goal of this paper was not to find the optimal dosage for the drugs, but to confirm the effectiveness of electroporation combined with classic chemotherapeutic drugs, and CaEP as a novel addition, on HepG2 cells. By using similar literature, and adding a few higher and lower concentrations, the test range of the dosage needed for an effective treatment could be limited.
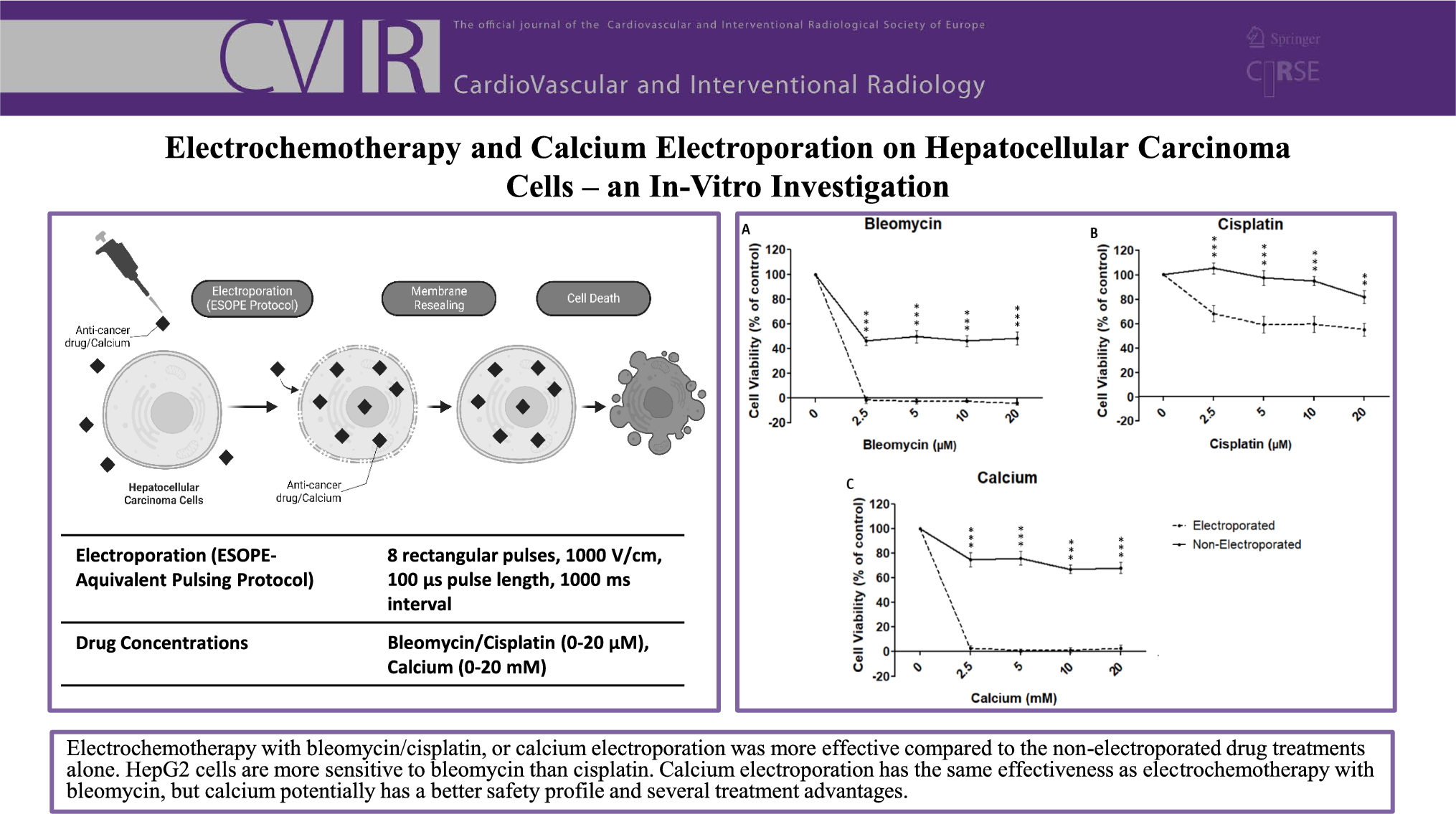
For all administered concentrations of bleomycin, cisplatin, or calcium, the combination with electroporation was more effective (minimum 27% and maximum 75% difference) in reducing the HepG2 cell viability compared to the non-electroporated controls, emphasizing the overall potential for ECT and CaEP. In general, to treat tumors with the same efficiency, ECT and CaEP use less drugs than conventional chemotherapies. This is in line with literature, as electro-permeabilization studies with classic chemotherapeutics have reported an enhanced cytotoxicity up to several thousand-fold for bleomycin, and up to 80-fold for cisplatin due to an increased cellular uptake and accumulation of the drug [27, 28]. Moreover, our results also show that, within the same concentration range, ECT with bleomycin is more effective than with cisplatin to reduce HepG2 cell viability. Thus, supporting the role of bleomycin as the chemotherapeutic drug of choice for traditional ECT.
ECT with bleomycin and CaEP had a similar effect on HepG2 cell viability, reaching (almost) complete cell death in the lowest concentration of 2.5 µM and 2.5 mM, respectively. Further concentration increase of the drugs did not cause any significant changes. However, it has been reported that 10 µM bleomycin and 5 mM calcium are considered to be the optimal concentrations in vitro as they cause 80% cell death [19, 21, 24, 25]. This suggests that the HepG2 cells within our study were more sensitive to both drugs in combination with electroporation. This underlines that more research is needed to optimize the drug concentrations for different cell types. It has been reported that several physical and biological cell properties can affect electroporation efficiency. [12, 29]
Despite their equal effectiveness combined with electroporation, bleomycin and calcium display different cytotoxic profiles when used as drug alone without electroporation. Calcium alone caused a reduction of HepG2 cell viability to 75%, compared to 46% for bleomycin, this suggests that CaEP is an equally effective but safer option. Similar studies, for different cell lines, have even reported that calcium alone had no significant impact on cell viability in comparable concentrations up to 20 mM. [12, 19, 30] Initial clinical studies have also found high doses of calcium (220–225 mM) to be well tolerated, contrary to classic chemotherapeutics. [22, 31]
Besides calcium’s potentially good safety profile, especially for patients, but also for the staff handling the drug, it is efficient, easily available, inexpensive, heat-stable and has a long shelf life [32]. This shows that CaEP, compared to traditional ECT, has the potential to be an applicable treatment for high-, middle, and low-income countries.
In this study, the HepG2 cell line was again chosen for experiments because of its good representation of the patient population with liver cancer treated in our department, where the majority classifies as Caucasian male, and in literature [23]. However, the previously used cell suspension setup, designed in our department, was replaced by classic EP cuvettes. Together with the ESOPE-protocol, of which the RE effectiveness had been previously proven for the HepG2 cell line (Fig. 2), it allowed for better comparison with relevant literature. An effect of pH and temperature changes due to pulsing on cell viability can be excluded in this study. As before, pH changes were minimized by using stainless-steel electrodes and a buffered, low-conductivity solution. In addition, the ESOPE protocol has shown not to significantly change the temperature of the samples. [23]
However, there are some limitations to the used methods. During (almost) complete cell death, some HepG2 cell viability values (ECT with bleomycin) measured by the MTT assay, appeared to be negative. However, there was no significant difference between the positive and negative values, resulting in an overall 0% cell viability. Some values exceeded 100% viability (2.5 µM cisplatin non-electroporated). This specific treatment might have stressed the cells, causing an increase in their metabolism as a response, detected by the MTT assay [33]. In addition, to get an initial idea about the suitable IRE and RE pulse parameters, and the efficacy of ECT and CaEP, the initial study as well as this follow-up study have been performed in vitro using HepG2 cells. As IRE and ECT work in cell suspension as well as in deep seated tumors, in vitro studies for CaEP with hepatic cell lines are an important indicator and basic prerequisite for animal experiments. As limitation, these results are not directly translatable to the clinic, as the in vivo environment is more complex.
To conclude the current study, ECT with bleomycin or cisplatin, or CaEP were more effective in reducing the HepG2 cell viability in vitro using the ESOPE protocol compared to the non-electroporated drug treatments alone. When comparing ECT, HepG2 cells are more sensitive to bleomycin than cisplatin, in similar concentrations. CaEP has the same effectiveness as ECT with bleomycin, but calcium potentially has a better safety profile and several treatment advantages. Despite these promising results, more research is needed to transfer CaEP as novel cancer treatment to the clinic, and to extend the application of traditional ECT to deep-seated tumors like liver cancer.



留言 (0)