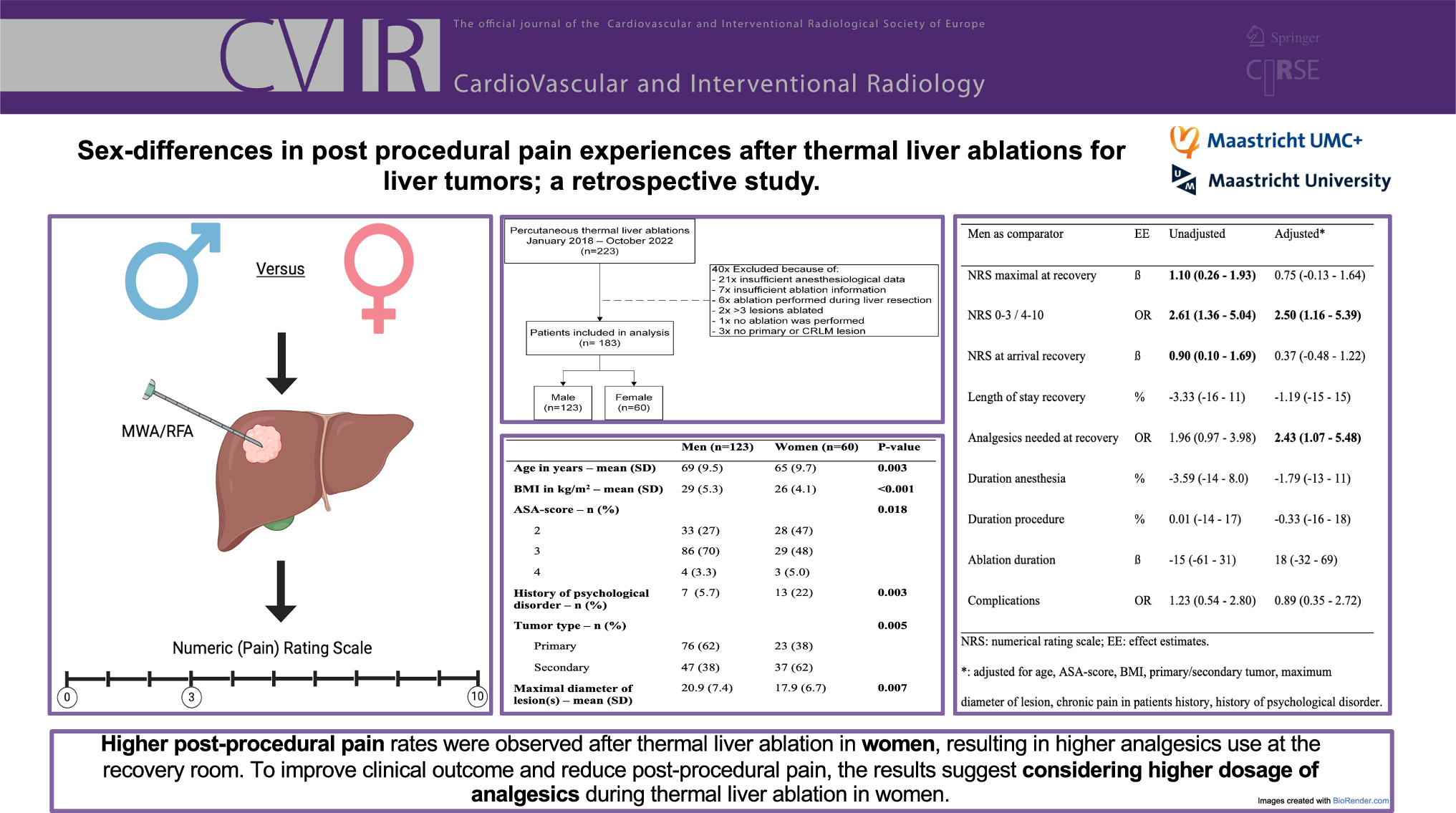
This study investigated pain experiences after thermal liver ablation between men and women. Women experienced higher maximum pain scores, had more often moderate to severe pain, and needed more often analgesics in the recovery room for pain treatment.
On the NRS, women exhibited a higher average maximal pain intensity (3.88 versus 2.73) and a higher prevalence of post-ablation pain (NRS 4–10) compared to men. It has been considered that a minimum change of 1.39 in NRS score is clinically relevant, meaning that our difference in maximal pain intensity might not reach this threshold [14]. However, an NRS ≥ 4 may be more clinically relevant because these patients potentially need pain treatment [15]. This substantiates our results, since women suffered more from postablation pain and needed analgesia more often post-procedurally. Altogether, this data suggests that sex is a relevant post-ablation pain predictor, urging anesthesia care providers to consider it during the procedure to reduce post-ablation pain.
A prior study found higher pain intensities immediately after thermal ablation in patients treated for HCC within two centimeters of the parietal peritoneum [13]. The parietal peritoneum was defined as the abdominal wall at a level below the main portal bifurcation. Above this level, it was defined as the diaphragm, which was not associated with higher pain experiences (P = 0.90) [13]. In our study, women were equally exposed to subcapsular tumors compared to men (52% versus 49%; Table 1), limiting the potential influence of tumor location on the pain intensities. Besides, univariable analysis showed no association between the location of the tumor and post-procedural pain.
In general, a larger ablation zone is desired in patients with CRLM, requiring a more aggressive thermal ablation [2, 16]. This may influence the pain intensity in patients, since larger ablation volumes are related to post-ablation pain [12]. In our study, women suffered more from metastases compared to men (38% versus 62%), potentially explaining the higher pain intensity levels. However, there was no significant interaction term between the maximal NRS score and the tumor type, suggesting a limited effect of tumor type on pain intensity. Additionally, we adjusted for tumor type in our regression model to minimize this potential effect.
In surgical settings, pre-operative pain predictors are well-studied. As mentioned earlier, various factors, such as female sex, smoking, higher BMI, younger age, anxiety, history of pre-operative pain, and expectations of post-operative pain, are known to have a negative relation with post-operation pain control [10, 11, and 17]. In our study, besides female sex, history of pre-operative pain, and psychological disorder were potential pain predictors. The reason for this might be the limited influence of such factors in minimally invasive procedures compared to liver surgery on post-procedural pain. During thermal liver ablation, three moments are known to cause pain: skin puncture, liver capsule puncture, and thermal energy transfer [18]. It is conceivable that the number of pain events is significantly higher in liver surgery. This might result in the release of higher levels of inflammatory mediators in liver surgery compared to minimal invasive thermal liver ablation. Such mediators activate peripheral nociceptors and cause peripheral and central sensitization, leading to acute and post-operative pain [19, 20]. When lower amounts of mediators are released, fewer factors may influence this sensitization, thus causing post-procedural pain.
Multiple studies have compared different sedation techniques and analgesics during thermal liver ablations. One study showed lower post-ablation pain in patients treated with intravenous oxycodone versus fentanyl [21]. A Chinese study compared remifentanil plus propofol versus oxycodone and found lower visual analog scale (VAS) scores in patients treated with remifentanil and propofol, whereas another study showed lower VAS scores in patients treated with propofol sedation or general anesthesia versus midazolam sedation [22, 23]. These results suggest that different anesthesia techniques and analgesics result in different post-ablation pain experiences, rendering the comparison of experienced pain very difficult. In our study propofol sedation in combination with a short acting opioid (in most cases remifentanil) was used in the majority of the patients. No statistically significant differences were observed in the use of analgesics between women and men except for metamizole, see Table S2. Metamizole was used more in women compared to men (8.3% versus 0.0%, P < 0.01). The higher use of metamizole during thermal ablation may explain the higher post-procedural pain scores in women.
The reasons why women and men experience different levels of pain are still an ongoing research topic. Sex hormones, genotype, and endogenous opioid function may all play a potential role in these differences in pain experiences [24]. A meta-analysis reported sex-specific differences in morphine-induced pain treatment, with women responding better. However, most studies included in this meta-analysis have focused on opioid consumption rather than pain relief [25]. Until more aspects have been thoroughly investigated, anesthesia care providers need to consider post-procedural pain differences in women undergoing thermal liver ablation. They should consider higher dosages of analgesics, possible morphine acting opioids, to reduce post-procedural excessive pain.
Some limitations must be mentioned. First, this single-center study used retrospectively collected data with a subjective pain measurement. Secondly, anesthesia care providers were free to choose different analgesics during the thermal ablation procedure, potentially causing inconsistent sedation levels. As shown above, comparable medications, dosage, and sedation techniques were used in both groups, and the distribution of men and women was equal among treating anesthesia care providers minimalizing this potential bias. Thirdly, some bias may occur, since two different ablation systems were used, the influence of these different ablation techniques could not be taken into account. However, Table S4 shows no difference in the proportion of men or women treated with each ablation system, therefore influence is probably limited.



留言 (0)