Appendix A, Table 1 illustrates the quantitative results of the questionnaire. Per topic, the results of the questionnaire and FGD are summarized.
Standardization
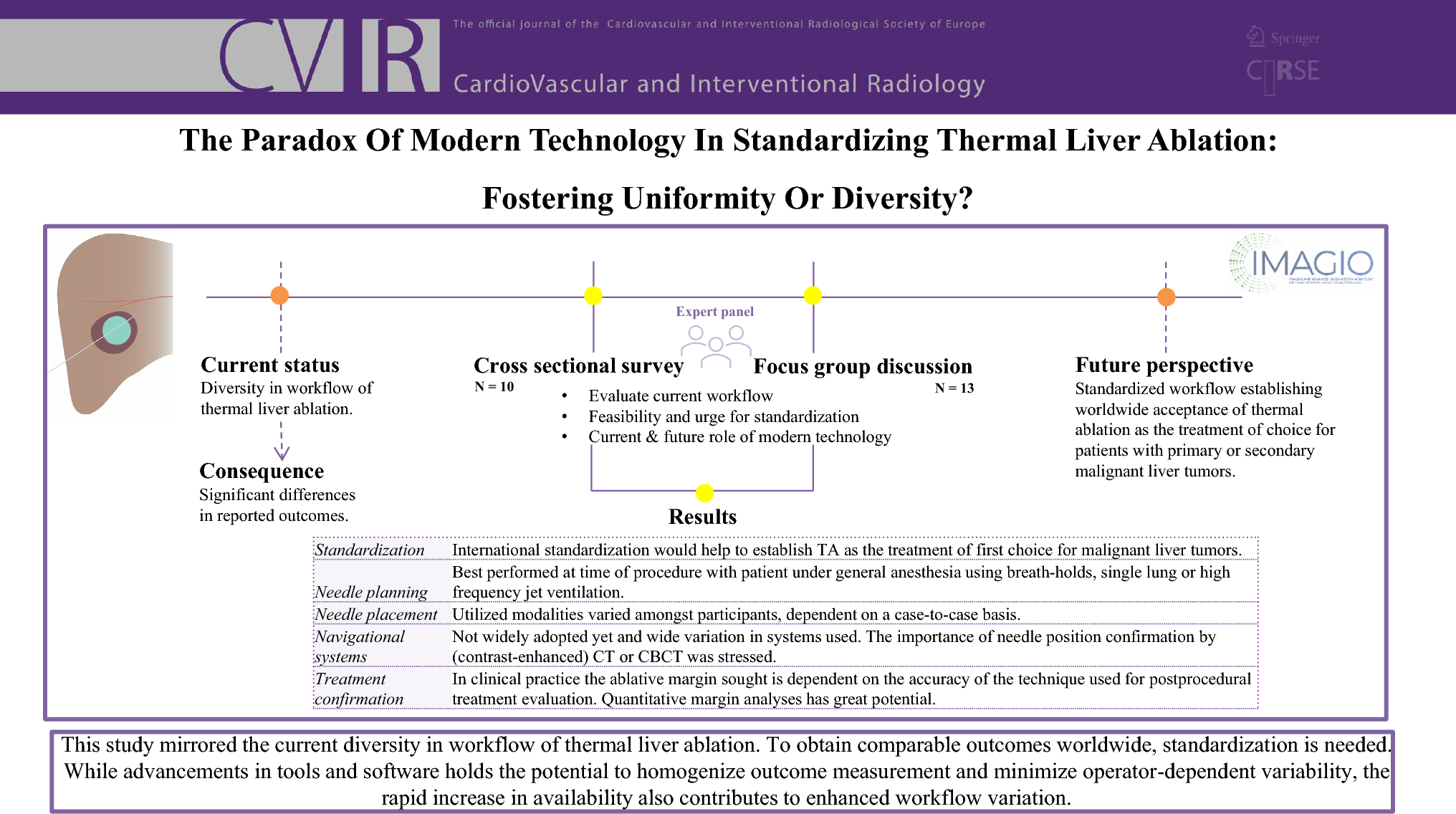
Nine respondents emphasized the importance of international standardization of liver tumor ablation, while one respondent did not due to the unclear specification of the proposed standardization. During the FGD, there was consensus that standardization would help to establish TA as treatment of first choice for malignant liver lesions. To compete with surgery, TA should universally be excellent with limited operator-dependency. Participants noted that some standardization already exists through guidelines from CIRSE, the Society of Interventional Radiology and the Society of Interventional Oncology.
Software-assisted Preprocedural Planning
The FGD revealed that all participants currently use preprocedural cross-sectional computed tomography (CT) and/or magnetic resonance imaging images for patient selection and needle trajectory planning. There was consensus that needle planning is best performed periprocedural, preferably with the patient under general anesthesia using respiratory control (i.e., breath-holds, single-lung or high-frequency jet ventilation). It was stressed that the position and morphology of the liver depend on the patient’s position and breathing and thus may vary considerably. Software-assisted planning prior to the intervention using pre-procedural images was therefore considered of limited use. Pre-procedural planning software, however, could be beneficial in hands-on simulation training for trainees and inexperienced interventional radiologists.
Needle Placement
Four of the respondents considered ultrasonography (US) as the modality of first choice as it allows real-time needle placement. In the event of poor visibility on US, additional modalities are required. During the FGD, there was consensus that image fusion could facilitate the localization and targeting of those lesions. Also, it was stated that the choice of the imaging modality, used for needle placement, depends on a case-by-case basis.
Navigational Tools
Four of the respondents integrated advanced navigational systems from seven different vendors into their clinical practice, while two respondents were exclusively using them within research projects. Considering the static nature of the CT-images that are currently being used for needle navigation, the importance of respiratory control and potential inaccuracies that arise from alternating liver morphology were once again highlighted during the FGD. There was a widespread agreement that confirming needle position and post-ablation margins with contrast-enhanced (cone bean) CT are crucial for optimization of outcomes.
Treatment Confirmation
To assess technical success, six of the respondents primarily used side-by-side visual (‘eye-balling’) qualitative assessment. Two respondents used visual three-dimensional assessment of ablative margins via pre- and post-ablation CT coregistration. The remaining two respondents employed quantitative assessment of the ablative margins with coregistration. The FGD considered quantitative margin analyses as a method with great potential, but further research is required before it can be widely implemented for clinical decision-making.



留言 (0)