
記住我




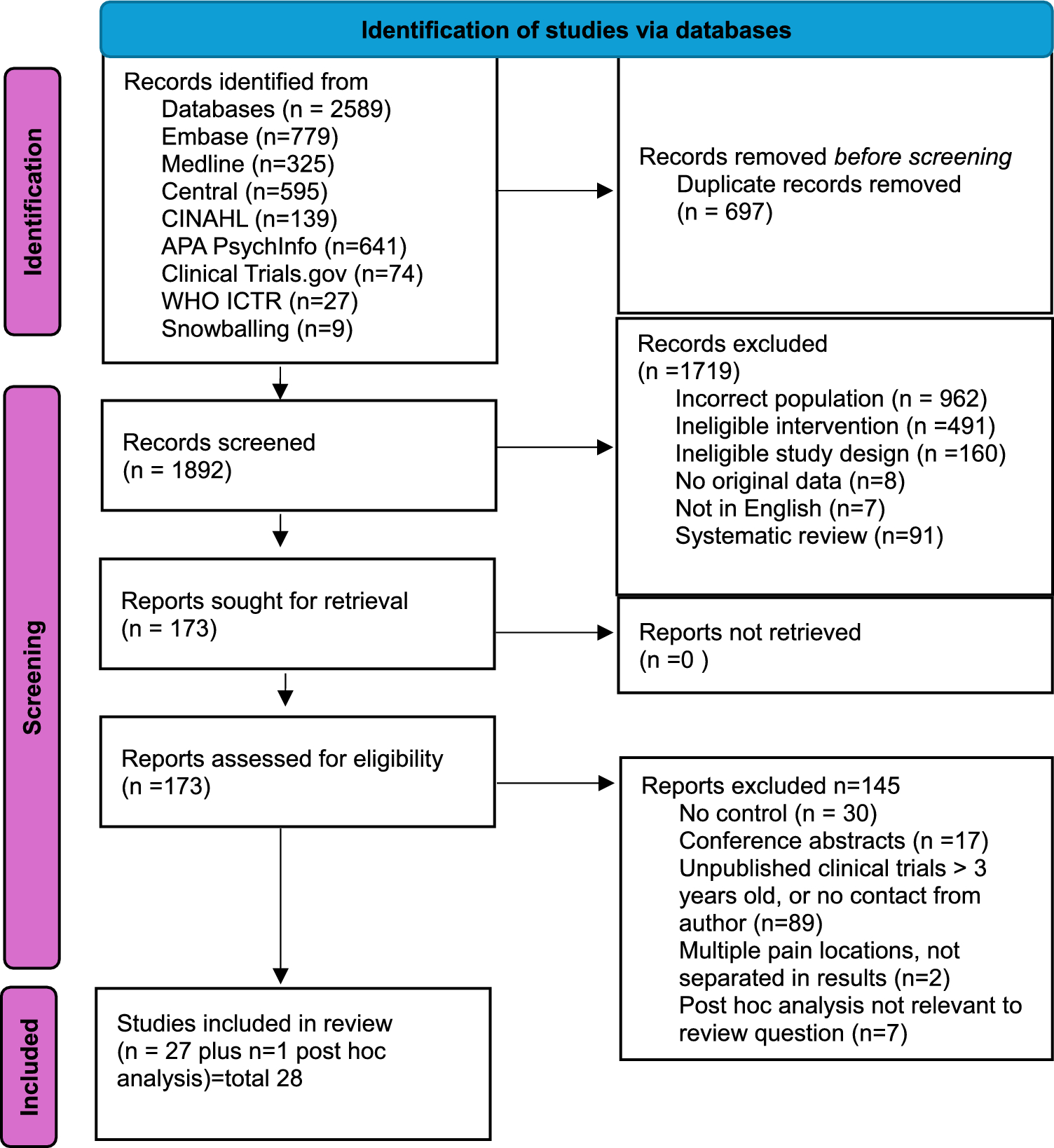
A total of 9407 records were identified by the search in the electronic databases and other sources (Fig. 1). After removal of exact duplicates and screening of title and abstract, 161 full-text articles were assessed for eligibility. Eventually, 44 articles were included in our analysis: 11 articles on patients with coronary disease, 29 articles on patients with stroke or TIA, and 4 articles on patients with peripheral arterial disease. Moreover, three studies (two RCTs and one post hoc analysis of an RCT) in patients with stroke or TIA involving only CYP2C19 LOF carriers were identified. The main results of these three studies were described separately.
Fig. 1 3.1 Coronary Disease
3.1 Coronary DiseaseEleven RCTs comparing genotype-guided and standard antithrombotic treatment were included (Table 1) [14,15,16,17,18,19,20,21,22,23,24]. These 11 RCTs contained a total of 11,740 patients (range 60–5276). Of these 11,740 patients, 5958 were treated with genotype-guided treatment and 5782 with standard antithrombotic treatment.
Table 1 Characteristics of studies on coronary artery diseaseIn three RCTs, the study population consisted of patients with acute coronary syndrome or stable coronary artery disease [17, 18, 22]. Of the remaining eight RCTs, seven studies included only patients with acute coronary syndrome [14,15,16, 19, 20, 23, 24], and one study included only patients with stable coronary artery disease [21]. Furthermore, performance of percutaneous coronary intervention (PCI) was part of the inclusion criteria in nine RCTs [14, 15, 17,18,19, 21,22,23,24]. In the other two RCTs, not all patients underwent a revascularization procedure: in the PHARMCLO study, 62% underwent a PCI and 11% coronary artery bypass grafting [16], and in the study of Tam et al., 77% underwent a PCI and 4% coronary artery bypass grafting [20].
The drug regimens used as genotype-guided and standard treatment differed between the studies. In most RCTs, LOF carriers in the genotype-guided arm were treated with ticagrelor or prasugrel and non-carriers with clopidogrel. However, Xie et al. prescribed a double dose of clopidogrel in intermediate metabolizers and a combination of double-dose clopidogrel and cilostazol in poor metabolizers [23], Zhang et al. prescribed a double-dose of clopidogrel in intermediate metabolizers [24], and Tomaniak et al. used a treatment regimen with prasugrel for 1 week followed by therapy de-escalation to clopidogrel in LOF carriers [21]. In the standard treatment arm, most patients were treated with clopidogrel ± aspirin, except in the POPular genetics study, which used ticagrelor or prasugrel [15], and the PHARMCLO study [16], the ADAPT PCI study [22], and the study from Shi et al. [19], in which the choice of antiplatelet therapy was decided by the treating physician. Definitions of MACE and major bleeding differed among the included studies (Table 2).
Table 2 Definitions of outcome measurements in studies on coronary artery disease3.1.1 Risk of Bias AssessmentSome concerns on the risk of bias due to deviations from intended interventions were noted in all studies and some concerns on the risk of bias in selection of the reported result in two studies (Fig. 2). In none of the studies, a high risk of bias was found. Overall, nine studies were classified as low risk for bias and two studies raised some concerns.
Fig. 2
Risk of bias assessment in studies on coronary artery disease. The risk of bias was assessed with the Cochrane collaboration’s risk of bias tool for randomized trials
3.1.2 Clinical OutcomesCompared with standard antithrombotic treatment, genotype-guided therapy significantly reduced the risk of MACE (RR 0.60, 95% CI 0.43–0.83, I2 71%), myocardial infarction (RR 0.53, 95% CI 0.42–0.68, I2 0%), and stent thrombosis (RR 0.64, 95% CI 0.43–0.94, I2 0%) (Fig. 3). No significant differences between treatment groups were observed in the rate of cardiovascular death (RR 0.69, 95% CI 0.40–1.20, I2 57%), stroke (RR 0.65, 95% CI 0.42–1.01, I2 0%), and major bleeding (RR 0.93, 95% CI 0.70–1.23, I2 0%).
Fig. 3

Forest plots for the ischemic and bleeding outcomes in studies on coronary artery disease
Comparable results were found for all thrombotic and bleeding outcomes in a subgroup analysis excluding the two RCTs that raised some concerns (Supplementary Fig. 1), in a subgroup analysis on the nine RCTs that included only patients in whom a percutaneous coronary intervention was performed (Supplemental Fig. 2), and in a subgroup analysis that excluded the only RCT using a genotype-guided de-escalation strategy (POPular Genetics) (data not shown). In a subgroup analysis based on studies with a follow-up duration of 12 months or more and in a subgroup analysis on studies including only patients with acute coronary syndrome, the risk of stent thrombosis did not differ significantly between genotype-guided and standard antithrombotic treatment (RR 0.68, 95% CI 0.46–1.02, I2 0%, and RR 0.63, 95% CI 0.39–1.01, I2 0%, respectively) (Supplementary Figs. 3d and 4d). A significantly decreased risk of stroke was found in the subgroup analysis on studies including only patients with acute coronary syndrome (RR 0.56, 95% CI 0.33–0.97, I2 0%) (Supplementary Fig. 4e).
3.2 StrokeA total of 29 studies describing the association between CYP2C19 genotype status, and clinical outcomes were eligible for inclusion in our analysis [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]. Of these 29 studies, 22 were cohort studies and 7 were post hoc analyses of RCTs. Characteristics of these studies are described in Table 3.
Table 3 Characteristics of studies on stroke or TIAThe 22 cohort studies contained a total of 5182 patients (range 42–743), and the seven post hoc analyses of RCTs contained 3356 patients (range 112–1463). In seven studies, both ischemic stroke and TIA patients were included [27, 28, 35, 36, 41, 46, 47]. One of these studies specified ischemic stroke as symptomatic small subcortical stroke [35]. Two studies only included patients who received a cerebrovascular stent because of atherosclerotic stenosis [30, 50]. In the study of Patel et al., only patients with asymptomatic extracranial carotid artery stenosis were included, and these patients were divided in a medical therapy cohort and a procedural cohort [38]. In the remaining 19 studies, only patients with history of ischemic stroke were included [25, 26, 29, 31,32,33,34, 37, 39, 40, 42,43,44,45, 48, 49, 51]. Definitions of MACE and bleeding differed among the included studies (Table 4).
Table 4 Definitions of outcome measurements in studies on stroke or TIA3.2.1 Risk of Bias AssessmentThe mean NOS score of included studies was 7.2 (Table 5). A total of 22 studies were scored as high quality studies (NOS score ≥ 7); 4 of these 22 studies were rated with the highest NOS score of 9. Seven studies had a NOS score < 7.
Table 5 Quality assessment (Newcastle–Ottawa Scale score) of studies on stroke or TIA3.2.2 Clinical OutcomesCarriers of a LOF allele had a significantly higher risk of MACE compared with non-carriers (RR 1.61, 95% CI 1.25–2.08, I2 62%) (Fig. 4). Moreover, the risk of ischemic stroke and all strokes was significantly higher in LOF carriers than in non-carriers (RR 1.89, 95% CI 1.48–2.40, I2 16% and RR 1.43, 95% CI 1.08–1.89, I2 0%, respectively).
Fig. 4

Forest plots for the ischemic and bleeding outcomes in studies on stroke or TIA
No significant differences were found in the risk of myocardial infarction (RR 1.09, 95% CI 0.37–3.20, I2 0%), major bleeding (RR 0.90, 95% CI 0.43–1.89, I2 0%), and all bleeding (RR 0.96, 95% CI 0.70–1.32, I2 0%). Subanalyses including only high-quality studies with a NOS score ≥ 7, studies with a duration of follow-up longer than 12 months, and only the post hoc analyses of RCTs demonstrated robust results (Supplementary Figs. 5, 6, and 7).
3.2.3 RCTs Including Only LOF Carriers: Description of Main ResultsIn our full-text screening, two RCTs involving only CYP2C19 LOF carriers were identified. The CHANCE-2 trial was a double-blind, placebo-controlled RCT among mainly Han Chinese patients (98%) with an acute minor ischemic stroke (NIHSS score ≤ 3) or high-risk TIA (ABCD2 score ≥ 4) [52]. Patients were randomized to receive ticagrelor or clopidogrel through day 90. All patients received aspirin for 21 days. A total of 3205 patients were assigned to the ticagrelor group and 3207 to the clopidogrel group. Patients who were treated with ticagrelor-aspirin had a significantly lower risk of a new ischemic or hemorrhagic stroke within 90 days compared with patients with clopidogrel–aspirin [6.0% versus 7.6% respectively; hazard ratio (HR) 0.77, 95% CI 0.64–0.94]. Ticagrelor increased the risk of any bleeding compared with clopidogrel (5.3% versus 2.5% respectively, HR 2.18, 95% CI 1.66–2.85). A post hoc analysis showed that these bleedings were generally mild and occurred mostly in the first 21 days after randomization [53]. No significant differences were found in the risk of severe or moderate bleeding (both 0.3%, HR 0.82, 95% CI 0.34–1.98) [52].
Another RCT included only single CYP2C19 LOF carriers (*1/*2, *1/*3) with an acute minor ischemic stroke (NIHSS score ≤ 5) and moderate-to-severe cerebral artery stenosis (> 50%). Patients were randomly assigned to receive a combination of high dose clopidogrel (150 mg per day) and aspirin (100 mg per day) or a combination of normal dose clopidogrel (75 mg per day) and aspirin (100 mg per day). After the first 21 days, clopidogrel was stopped and monotherapy with aspirin was continued during the 90-day observation period. In total, 62 patients with high dose clopidogrel and 69 patients with normal dose clopidogrel were analyzed. No significant differences in the vascular event rate were found between these two treatment groups [54].
3.2.4 RCT Comparing Genotype-Guided with Standard TreatmentOur full-text screening identified one RCT that compared a personalized genotype-guided treatment strategy with standard treatment. In this RCT, 650 adult patients with a mild-to-moderate acute noncardioembolic ischemic stroke (NIHSS ≤ 5) or a moderate-to-high risk TIA (ABCD2 score ≥ 4) were included from 2019 to 2021 in China [55]. Patients were randomized in a pharmacogenetic or standard treatment group. In the pharmacogenetic group, all patients were treated with aspirin (until day 90). Ultrarapid (*17/*17), rapid (*1/*17), and extensive (*1/*1) metabolizers were also treated with clopidogrel 75 mg/day, intermediate (*1/*2, *1/*3, *17/*2, *17/*3) metabolizers with clopidogrel 150 mg/day, and poor (*2/*2, *2/*3, *3/*3) metabolizers with ticagrelor 90 mg twice daily (until day 21). The standard group was treated with aspirin (until day 90) and clopidogrel 75 mg/day (until day 21). After a 90-day follow-up, patients in the pharmacogenetic group had a significantly lower risk of new stroke (RR 0.27, 95% CI 0.08–0.97) and composite vascular events (RR 0.38, 95% CI 0.16–0.92). No differences in major bleeding were found between treatment groups (RR 1.50, 95% CI 0.25–8.95) [55].
3.3 Peripheral Arterial DiseaseAfter full-text screening, four studies were eligible for inclusion: a retrospective study [56], a prospective study [
留言 (0)