
記住我



A total of 933 (89.0%, 933/1048) qualified sequences were obtained, representing 82.6% (933/1129) newly diagnosed HIV-positive patients in Shaoxing city from 2019 to 2023. As shown in Table 1, the patients were mainly male (82.1%, 766/933) and local residents (84.1%, 785/933); 52.9% (494/933) of patients were married, 33.8% (315/933) had a junior middle school education, 61.8% (577/933) were infected through heterosexual contact, and 48.1% (449/933) were infected with the CRF07_BC subtype. A total of 38.3% (357/933) of the individuals were older than 50 years, and the median age for the entire cohort was 44 years (ranging from 18 to 81 years). There was a significant difference in the composition of subtypes between the ≥ 50-year-old group and the < 50-year-old group (χ2 = 36.929, P < 0.001).
Table 1 Sociodemographic Characteristics of newly diagnosed HIV-1 patients in Shaoxing from 2019 to 2023HIV subtype distributionTwelve HIV-1 subtypes and a proportion of unique recombinant forms (URFs) were identified from the 933 pol sequences. CRF07_BC was the predominant subtype, accounting for 48.1% (449/933) of sequences, followed by CRF01_AE (29.4%, 274/933). The other subtypes detected were CRF08_BC (11.3%, 105/933), CRF85_BC (3.3%, 31/933), CRF55_01B (2.5%, 23/933), B (1.4%, 13/933), C (0.8%, 7/933), CRF87_cpx (0.3%, 3/933), CRF57_BC (0.2%, 2/933), 02_AG (0.1%, 1/933), URF (CRF01_AE/CRF07_BC) (2.47%, 23/933), URF (CRF01_AE/B) (0.1%, 1/933), and URF (B/C) (0.1%, 1/933).
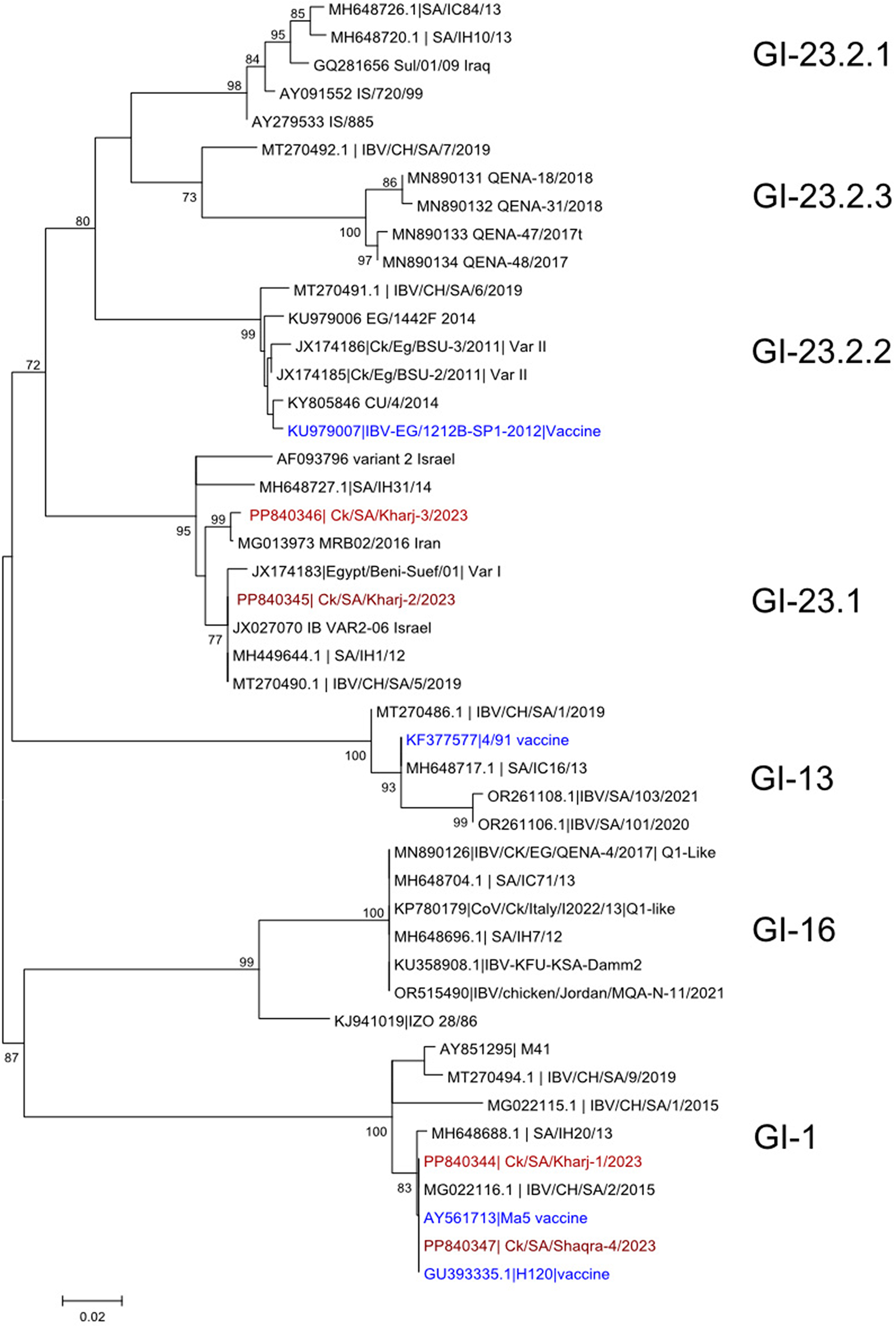
By constructing the ML phylogenetic trees of the different HIV-1 subtypes (Fig. 1), we found that there was a large evolutionary clade in the CRF07_BC subtype named C1. A total of 94.2% (65/69) of the CRF07_BC-C1 individuals were infected through heterosexual contact, 88.4% (61/69) were older than 50 years, and 88.4% (61/69) were drug resistant. CRF01_AE in Shaoxing city was homologous to several CRF01_AE epidemic clusters in China. The major subclusters were CRF01_AE Cluster1 (23.7%, 65/274), CRF01_AE Cluster4 (19.3%, 53/274) and CRF01_AE Cluster5 (8.6%, 24/274). The other detected subclusters were CRF01_AE Cluster8 (1.5%, 4/274), CRF01_AE Cluster2 (1.5%, 4/274), and CRF01_AE Cluster3 (1.8%, 5/274). Individuals in the largest subcluster, CRF01_AE Cluster1, were mainly infected through heterosexual transmission (95.4%, 62/65), and 63.1% (41/65) of the patients were over 50 years old. In addition to the two major HIV-1 subtypes, the other HIV-1 subtypes were concentrated among heterosexual individuals (81.0%, 170/210).
Fig. 1
Maximum-likelihood phylogenetic trees of patients infected with different HIV-1 subtypes in Shaoxing city from 2019 to 2023. The phylogenetic trees based on the pol region of different HIV-1 subtypes were constructed by an approximate maximumlikehood method with IQ Tree 2.0.6 under the GTR+G+I nucleotide substitution model. Clades of different colours represent different HIV-1 subtypes and subclusters. The inner circle red colour square box represents ressistances individuals; the outer circles shows the risk group, Black colour square box represents heterosexual individuals, White colour square box represents homosexual individuals. A Maximum-likehood phylogenetic tree of CRF07_BC. B Maximum-likehood phylogenetic tree of CRF01_AE.C Maximim-likehood phylogenetic tree of other HIV-1 subtypes.
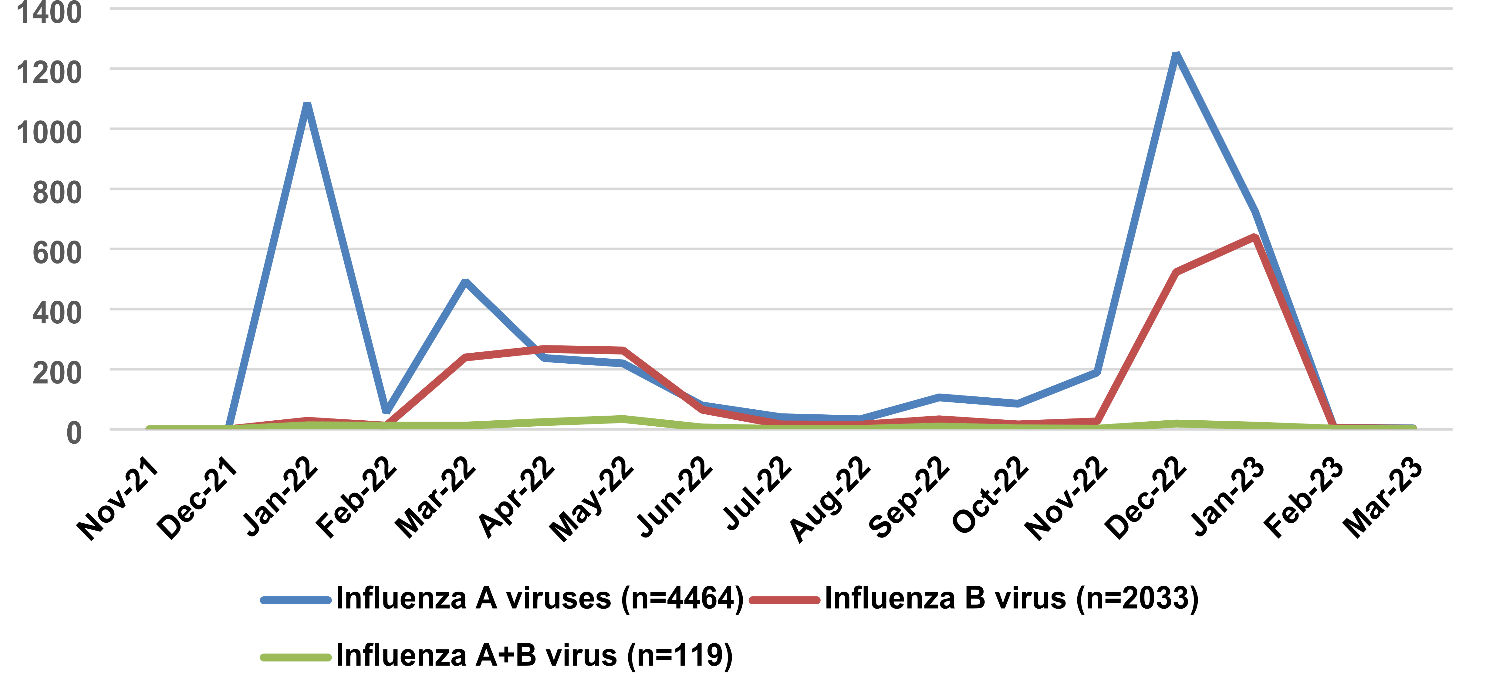
Genetic transmission network analysisAt the optimal GD of 0.0075 substitutions/site, 398 individuals (42.7%, 398/933) formed 98 clusters (mean 4.1, median 2.0, range 2–64, interquartile range 2–3.75) and 1534 edges (mean 7.7, median 3.0, range 1–59, interquartile range 1–5) (Table 2 and Fig. 2). Among the 98 clusters, the subtypes included CRF07_BC (51.3%, 204/398), CRF01_AE (22.4%, 89/398), CRF08_BC (15.3%, 61/398), CRF85_BC (6.0%, 24/398), CRF55_01B (2.5%, 10/398), B (1.0%, 4/398), C (1.0%, 4/398) and URF (CRF01_AE/CRF07_BC) (0.5%, 2/398). There were 4 LCs (4.1%, 4/98), 21 MCs (21.4%, 21/98), and 73 SCs (74.5%, 73/98). Eight MCs clustered patients who were diagnosed after 2021, and 18 clusters exhibited an increasing number of cases ≥ 3 from 2021 to 2023. CRF07_BC formed the most clusters (nodes ranging from 2 to 64) in the network. We also observed that 21.4% (85/398) of the PDR patients were included in the transmission network. A total of 65.9% (56/85) of the PDR patients were concentrated in the LC1 cluster (Table 2 and Fig. 2).
Table 2 Molecular network clustering of different HIV-1 subtypes in Shaoxing city from 2019 to 2023Fig. 2
Molecular transmission network analysis of patients infected with different HIV-1 subtypes in Shaoxing city from 2019 to 2023. All edges represent a genetic distance between nodes of less than 0.0075 substitution/site, and the colour of the node indicates the different HIV-1 subtypes. Different shapes denote sex, and the mode size indicates the number of associated links. Thick border represents resistances individuals.  Represents FSW individuals
Represents FSW individuals
The proportions of PDR in patients with different subtypes were 35.8% (73/204), 4.5% (4/89), and 7.6% (8/105) for CRF07_BC, CRF01_AE, and other subtypes, respectively. The proportion in the CRF07_BC subtype was significantly greater than those of the CRF01_AE and other subtypes (χ2 = 52.148, p < 0.001)(Fig. 2).
Of the four LCs, the CRF07_BC cluster (LC1) had 64 nodes, the CRF08_BC cluster (LC2) had 28 nodes, the CRF01_AE cluster (LC3) had 16 nodes and the CRF85_BC cluster (LC4) had 16 nodes (Fig. 2). All four LCs were defined as elder heterosexual infection clusters. A total of 124 nodes were identified; 93.5% (116/124) were predominantly infected through heterosexual contact, and 80.6% (100/124) were aged 50 years or older. There were 34 females, 52.9% (18/34) of whom were infected by spouses or regular sexual partners. In addition, 4 female sex workers (FSWs) from other provinces were included in these clusters, including two patients in LC1, one patient in LC2 and one patient in LC3. The largest cluster (LC1) contained 64 nodes, a mean of 33 edges (median 39, range 1–59, interquartile range 18–47), and a mean GD of 0.0051 (median 0.0052, interquartile range 0.0042–0.0062). Among the 64 patients, 90.6% (58/64) were local residents, 85.9% (55/64) had a junior middle school education or below, 93.8% (60/64) were infected through heterosexual transmission, 87.5% (56/64) were drug resistant, and 32.8% (21/64) were female; most females (66.7%, 14/21) were detected after their spouses or regular sexual partners were confirmed to be HIV positive. The characteristics of the four LCs are shown in Table 3.
Table 3 Summary statistics of the four largest Clusters in Shaoxing city from 2019 to 2023Factors associated with clustering and high linkagesOf the individuals included in the clusters, 78.6%(313/398) were male, 50.0%(199/398) were ≥ 50 years old, 59.5%(237/398) were married, 51.3%(204/398) were infected with CRF07_BC, 88.2%(351/398) were local residents, and 67.8%(270/398) were infected through heterosexual transmission (Table 4). Multivariate logistic regression analysis revealed that age, nationality, subtype, and PDR were the most significant factors associated with clustering in the transmission network (Table 4). Patients aged ≥ 50 years were more likely to cluster within the network (adjusted odds ratio [AOR] = 1.868, 95% confidence interval [CI] 1.329–2.625). We also found that individuals with PDR were more likely to cluster than those without PDR (AOR = 2.219, 95% CI 1.491–3.301). Individuals in other ethnic groups (AOR = 0.464, 95% CI 0.232–0.925) and with CRF01_AE (AOR = 0.678, 95% CI 0.487–0.944) had significantly lower odds of clustering than Han individuals and patients with CRF07_BC.
Table 4 Factor associated with clustering and high linkages of newly diagnosed HIV-1 patients in Shaoxing from 2019 to 2023We defined nodes with ≥ 4 links as high-risk individuals. Multivariate logistic regression analysis also revealed that age, subtype, and PDR were significant factors associated with high-risk individuals (Table 4). The results showed that the effect of age ≥ 50 years was 5.149 times greater than that of age < 50 years (95% CI = 2.689–9.859), that of individuals with PDR was 3.899 times greater than that of individuals without PDR (95% CI = 1.971–7.711), and that of CRF01_AE and other subtypes were 0.303 times (95% CI = 0.148–0.622) and 0.410 times (95% CI = 0.214–0.786) greater than that of CRF07_BC.
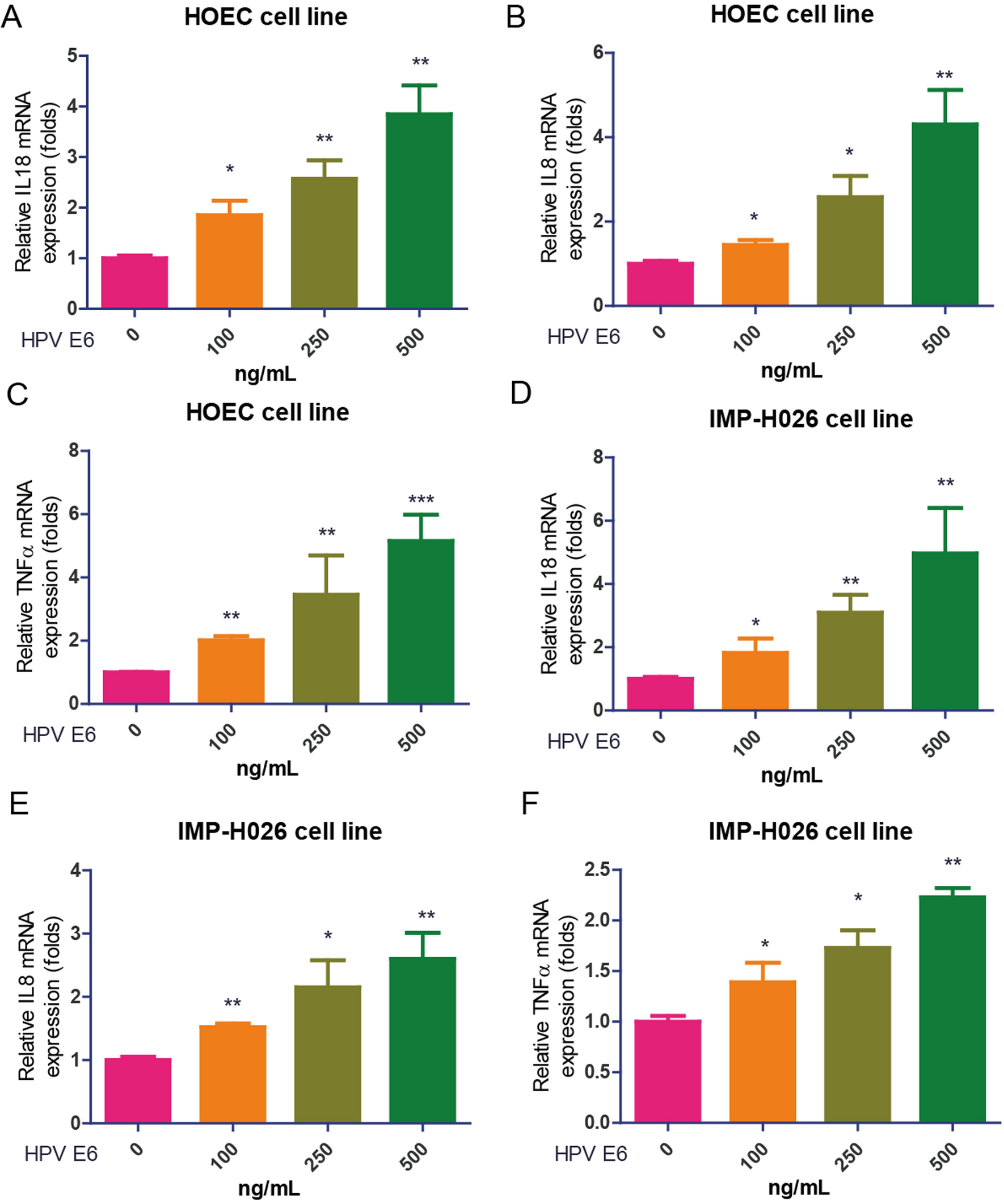
Drug resistance mutation analysisThe prevalence of PDR among newly diagnosed patients was 14.6% (136/933). Eleven protease inhibitor (PI) resistance-associated mutation patterns, 10 nucleoside reverse transcriptase inhibitor (NRTI) mutation patterns, and 13 non-nucleoside reverse transcriptase inhibitor (NNRTI) mutation patterns were identified. The overall prevalence of HIV-1 PDR to NNRTIs (10.0%, 93/933) was much greater than that to NRTIs (1.8%, 17/933) and PIs (3.2%, 30/933) (χ2 = 77.961, p < 0.001). In individuals with NNRTI resistance, the most frequent mutations were K103N/S/KN/NS (52.2%, 71/136), which were responsible for the greatest proportion of high-level resistance to nevirapine (NVP) and efavirenz (EFV) (52.2%). In individuals with PI resistance, resistance to tipranavir (TPV/r) was the most common (16.2%, 22/136), which was mainly related to the Q58E/QE mutation (14.7, 20/136)(Fig. 3). Four (2.9%, 4/136) strains harboured two classes of drug resistance mutations. No HIV-1 strains with PDR mutations to three classes of drugs were found in this study.
Fig. 3
A: Frequency of HIV-1 pretreatment drug resistance (PDR) mutations to PIs, NRTIs, and NNRTIs. B: Level of HIV-1 PDR associated mutations to different ART drug among 136 newly diagnosed HIV/AIDS patients. PI, Protease inhibitor; NRTI, Nucleoside reverse transcriptase inhibitor; NNRTI, Non-nucleoside reverse transcriptase inhibitor; ATV/r:Atazanavir/ritonavir; FPV/R:Fosamprenavir/ritonavir; IDV/r:Indinavir/ritonavir; LPV/r:Lopinavir/ritonavir; NFV:Nelfinavir; SQV/r:Saquinavir/ritonavir; TPV/r: Ritonavir/ritonavir; ABC: Abacavir; AZT: Zidovudine; D4T: Stavudine; DDI: Didanosine; FTC: Emtricitabine; 3TC, Lamivudine; TDF, Tenofovir; DOR, Doravirine; EFV, Efavirenz; ETR: Etravirine; NVP: Nevirapine; RPV: Rilpivirine
留言 (0)